
When University College Dublin virologist Dr Gerald Barry was interviewed by ‘The Irish Times’ and asked – why have we so many cases when we’re so highly boosted? – he said ‘Even asking the question points to the root of our problem in Ireland and in many parts of the world, we are using a tool that isn’t designed to stop infections and then wondering why it didn’t stop infections.’
‘I would strongly advocate for a complete reassessment of everything we have done to this point, identify everything else that could be done that would help, knock off everything that isn’t feasible or is unaffordable and do everything else.’
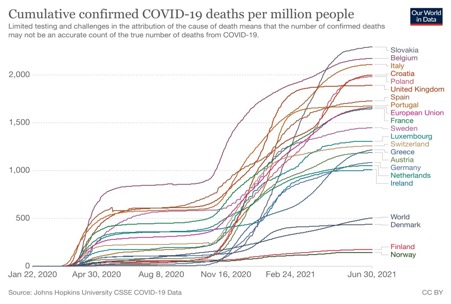
So we have failed? – ‘The problem with a “do more” strategy is that some countries that have demonstrably done less to curb the spread of infection, such as England, seem to be doing better overall.’
Just such a reassessment was recently reported in ‘The Guardian’ from Professor Mark Woolhouse, ‘one of the country’s leading epidemiologists’, who has written a forthcoming book, ‘The Year the World Went Mad: A Scientific Memoir’. Lockdown, he says, ‘was a lazy solution to a novel coronavirus epidemic, as well as a hugely damaging one”.
The day Britain went mad is reported as when ‘the No 10 briefing in March 2020, cabinet minister Michael Gove warned the virus did not discriminate. “Everyone is at risk,” he announced.’ To which Woodhouse responds: “I am afraid Gove’s statement was simply not true. In fact, this is a very discriminatory virus. Some people are much more at risk from it than others. People over 75 are an astonishing 10,000 times more at risk than those who are under 15.”
“We did serious harm to our children and young adults who were robbed of their education, jobs and normal existence, as well as suffering damage to their future prospects, while they were left to inherit a record-breaking mountain of public debt. All this to protect the NHS from a disease that is a far, far greater threat to the elderly, frail and infirm than to the young and healthy.”
“We were mesmerised by the once-in-a-century scale of the emergency and succeeded only in making a crisis even worse. In short, we panicked. This was an epidemic crying out for a precision public health approach and it got the opposite.”
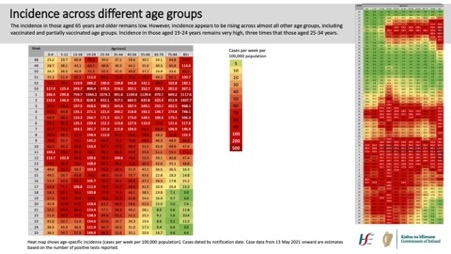
That Covid-19 is a disease that discriminates is a point made often on this blog and by others, which should have signaled that a blanket approach wasn’t warranted. A recent paper analysing this has recently been published, which shows the disparity in effect by age, despite the difficulties in measurement.
It records that in ‘Twenty-five seroprevalence surveys representing 14 countries were included . . . the median IFR [Infection Fatality Rate] in community-dwelling elderly and elderly overall was 2.9% (range 0.2%-6.9%) and 4.9% (range 0.2%-16.8%) . . . IFR was higher with larger proportions of people >85 years. Younger age strata had low IFR values (median 0.0013%, 0.0088%, 0.021%, 0.042%, 0.14%, and 0.65%, at 0-19, 20-29, 30-39, 40-49, 50-59, and 60-69 years . . .’
These IFRs have been calculated using data from 2020 and are therefore before widespread vaccination, at least in richer countries and before the less virulent Omicron variant. We can therefore expect these numbers to have fallen not only due to vaccination but also better hospital treatment as lessons began to be learned about ventilation etc. The paper notes that ‘absolute risk values still have substantial uncertainty’ and mentions the low number of elderly in the studies examined by the paper, but which might also reflect uncertainty about the total number of infections and number of deaths actually caused by Covid as opposed to deaths of people with Covid.
The link here to IFRs for various diseases shows that for the younger age groups Covid-19 is far down the list. According to the European Centre for Disease Prevention and Control here Influenza (over all ages) appears more severe than Covid-19 for those aged below 30 although this also depends on the virus, host issues, and other factors.
The paper also notes that ‘besides age, comorbidities and lower functional status markedly affects COVID-19 death risk. Particularly elderly nursing home residents accounted for 30-70% of COVID-19 deaths in high-income countries in the first wave, despite comprising <1% of the population. IFR in nursing home residents has been estimated to be as high as 25%.’
Professor Woolhouse argues in ‘The Guardian‘ article that:
‘the country should have put far more effort into protecting the vulnerable. Well over 30,000 people died of Covid-19 in Britain’s care homes. On average, each home got an extra £250,000 from the government to protect against the virus . . . “Much more should have been spent on providing protection for care homes,”
He ‘castigates the government for offering nothing more than a letter telling those shielding elderly parents and other vulnerable individuals in their own homes to take precautions,’ something this bloggers’ wife found particularly galling as medical personalities and politicians congratulated themselves and were congratulated by others for efforts on her and others’ behalf which consisted of nothing much more than a letter.
As ‘The Guardian’ goes on in reporting Woodhouse’s views – ‘The nation could have spent several thousand pounds per household on provision of routine testing and in helping to implement Covid-safe measures for those shielding others and that would still have amounted to a small fraction of the £300bn we eventually spent on our pandemic response, he argues. Indeed, Woolhouse is particularly disdainful of the neglect of “shielders”, such as care home workers and informal carers. “These people stood between the vulnerable and the virus but, for most of 2020, they got minimal recognition and received no help.”
The British Government, according to Woodhouse, thus “lacked a convincing plan for adequately protecting the more vulnerable members of society, the elderly and those who are immuno-compromised.”
“Lockdowns aren’t a public health policy. They signify a failure of public health policy.”
Back to part 1
Forward to part 3





 This week the Dáil debated
This week the Dáil debated  It’s almost as if someone has been reading these posts on the course of Covid-19 in Ireland. Fintan O’Toole’s latest
It’s almost as if someone has been reading these posts on the course of Covid-19 in Ireland. Fintan O’Toole’s latest  Following ‘the science’ and its scientists that we looked at in the two previous posts does not look well in hindsight, as a short review of the course of the pandemic in the Irish State demonstrates. In the early days these were forecasting 20,000 deaths, six times the current figure which is just over 3,300, and an even greater over-estimate than the influential Imperial College paper that forecast a possible 500,000 deaths in the UK.
Following ‘the science’ and its scientists that we looked at in the two previous posts does not look well in hindsight, as a short review of the course of the pandemic in the Irish State demonstrates. In the early days these were forecasting 20,000 deaths, six times the current figure which is just over 3,300, and an even greater over-estimate than the influential Imperial College paper that forecast a possible 500,000 deaths in the UK. The decision to attempt to prevent vaccines made in the EU getting to the UK via Northern Ireland led to a flurry of arguments that almost all mirrored the same nationalist impulse of the EU that was being criticised. This was true of some on the left as much as any other.
The decision to attempt to prevent vaccines made in the EU getting to the UK via Northern Ireland led to a flurry of arguments that almost all mirrored the same nationalist impulse of the EU that was being criticised. This was true of some on the left as much as any other. The view that there is a single scientific approach to the Covid-19 pandemic has had a number of consequences.
The view that there is a single scientific approach to the Covid-19 pandemic has had a number of consequences.