
The Irish State has reached the milestone of 5,000 deaths associated with Covid-19 at the same time as it controversially announced that there will not be a reopening of indoor hospitality on 5 July as planned.
Two weeks ago a government source had said that “the narrative that our reopening will slow down is not true.’ However that was before the National Public Health Emergency Team (NPHET) presented advice to it that a pessimistic ‘scenario’ forecasted 2,000 deaths over three months, largely due to the new Delta variant of the disease, with advice that only vaccinated people and those who have had Covid should be allowed inside restaurants etc.
Such a measure was denounced as ‘absolutely bananas” by one opposition leader amid accusations that it was unworkable, discriminatory and potentially illegal, never mind the damage to the social bond that arises from everyone making sacrifices together. Young people, it seemed, who predominantly serve in hospitality but are unvaccinated could serve, but not be served. Sinn Fein denounced the Government while more quietly accepting the decision; in this case talking more softly out of one corner of its mouth than the other. What would you do if faced with this dreaded forecast was the stock response from the governing parties.
While it was noted that NPHET had failed to factor into its assumptions newly allowed vaccination of younger people and there were calls for an independent audit of its modelling, plus claims that the Irish were an outlier in Europe in terms of indoor hospitality, by and large the figures were accepted without real challenge. The Irish State has had one of the strictest and longest lockdowns in Europe but if many more people are no longer so scared as they were, there is no alternative critical view of State policy beyond making it harder.
There are a number of reasons for this including that the Irish State has done relatively well in relation to deaths:
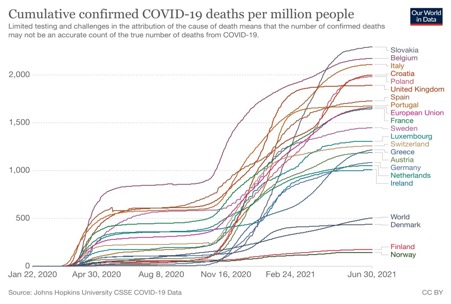
State support payments to the unemployed and businesses have continued, and political opposition, including from the left, has been in favour of even tighter restrictions. Such opposition as has declared itself, has been restricted to the far-right, including anti-Vaxxers who are easily dismissed but serve to make any other criticism easier to ignore.
The Irish economy is also set to grow by over 8%, according to the Central Bank, with this growth having less to do with base effects (the previous fall caused by lockdown making future growth easier statistically as well as economically) because the Irish economy has been hit less by Covid-19 despite the lockdown. The disproportionate presence of US multinationals, which includes companies in the pharmaceuticals, medical devices and IT sectors, has seen demand for their products increase.
An opinion poll in June reported that ‘fewer than one third of voters (32 per cent) agree that life should return “to the way it was before Covid” even after most people are vaccinated. Almost two-thirds (65 per cent) say that some precautions should remain in place, such as wearing masks in shops. Older voters remain significantly more cautious on this issue, with 79 per cent favouring continued precautions.’(Irish Times). The greater threat to older people goes a long way to explaining their particular concerns, as does the failure of the state to protect these people in its care or in private homes for which the state still has a responsibility.
That this number of people are so anxious is not a healthy sign, either from a psychological view or politically. A scared population is not one that is likely to be critical of state policy or seek to map out its own alternative. From a socialist viewpoint it is not conducive to independent thought by workers and rather affirms their social subordination. In this case the attendant denial of very basic civil liberties emphasises it.
Given the current very low level of cases, hospitalisation and deaths, plus the summer season, the dire warning by the Minister of Health, that “the biggest hurricane that has ever hit Ireland is coming’ simply reaffirms all these negative effects of state policy. Although one must assume his remark excludes An Gorta Mór.

The Government’s decision rests heavily on the most pessimistic of four scenarios presented by NPHET:

The presentation by NPHET shows a wide variation between a central scenario of 187,000 cases in three months and 545 deaths, and the pessimistic scenario of 682,000 cases and 2,170 deaths. Given the prevalence of the Delta variant, plus greater transmissibility by Alpha, it is the increase in social mixing that appears as the cause of the difference, but this is placing a big burden on indoor hospitality to make this the cause of such an increase. It is the possibility of the pessimistic scenario that is nevertheless given as the reason, although no probability is presented and the message appears to be that no possibility is acceptable.
The Chief Medical Officer has admitted that advice from his Scottish equivalent is that the Delta variant presents less risk of hospitalisation even if it is more transmissible. It is already well known that the virus is predominantly a threat to life to those who have other underlying health conditions.
The most recent figures published for the period up to 12 December 2020 report that 93.4% of deaths were of those with an underlying condition. The figures for those who had Covid-19 and also had an underlying condition was 16.9% for those aged 25 – 34, 52.58% for those aged between 65 and 74, and 59.4% of those 75+.
Clearly it is older people who are most at risk and it is mainly older people who are dying. The proportion of total deaths accounted for by 25 – 34 year-olds at 11 May 2021 was 0.81% while it was 15.5% for those aged 65 – 74, 33.75% for those aged 75 – 84, and 42.39% of those aged 85+. In other words, 91.64% of deaths were of those aged 65 and over, but being over this age is not sufficient to have a severe risk posed, you also need to have a relevant underlying condition.
NPHET has reported that cases amongst the eldest has fallen and lower than younger age groups, as this heat map shows:
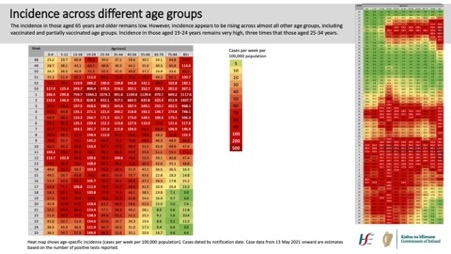
This is due in good part to the vaccination programme prioritising by age but also by considerations of those most vulnerable. The programme has also prioritised health care staff although this was supposed to be targeted to front line workers. In the North not so much pretence was made and back-office support workers with no interaction with patients were vaccinated before, for example, immunosuppressed cancer patients. The mantra of ‘protect the NHS’ reached a logical conclusion when bureaucrats came before extremely vulnerable patients. While the Southern vaccination programme has been beset by some scandal in which relatives of senior executives and others favoured by them have been vaccinated out of priority, the existence of similar in the North has gone unreported.
In both jurisdictions the unchallenged requirement for vaccination of health care staff arises because both health systems have been incapable of implementing effective infection control. In part this is because of the large number of Covid patients hospitalised but this in turn has been mainly due to the failure to protect older people, including those in care and nursing homes. The Irish Government Covid-19 hub reported, as an example, that on Tuesday 11 May over half of hospitalised cases were in the over 65 age group.
In any case, the vaccination programme has gone a long way to protecting those most vulnerable. Among these the rates of full vaccination are very high – 94% of those aged 80 and over, and 91% of those aged 70 – 79. Among the 60 – 69 age group 43% are fully vaccinated while 93% have had one dose. Around 68 per cent of all adults have had one dose of the vaccine, while 45 per cent have had full vaccination. This compares with Scotland where the incidence of infection, and by the Delta variant, has dramatically increased but existing relaxation of restrictions, including on indoor hospitality, have remained.
However, the argument of the government and NPHET is that the vaccination programme has not progressed sufficiently to reduce the risk and that it is younger people who must be increasingly targeted by the vaccination programme.
However, it is openly acknowledged that the dire warnings and continued restrictions are based on uncertainty about the possible number of cases, the number that will be hospitalised and the number of deaths. NPHET has forecast 2,170 in the next three months in its pessimistic scenario, but this would mean an over 40 per cent increase in the existing death toll in a very short period, one-fifth the time of the preceding pandemic. This, when the most vulnerable have received some sort of vaccination, so protecting them to a significant extent against both hospitalisation and death, and against a dominant variant we are informed involves less risk of hospitalisation.
There is a final reason to be wary of attempts to frighten the population and potentially introduce discriminatory measures against those who face least risk. Leo Varadkar has written ‘that Ireland is among a small number of countries that includes in our numbers suspected and probable deaths from Covid even when the patient did not test positive or was not tested at all.’
The Northern Ireland Statistics Research Agency has reported that:
‘There were 1,626 deaths registered up to 31st December 2020 where Covid‐19 was identified as the underlying cause of death (88.8% of the 1,831 Covid‐19 related deaths). For 157 out of these 1,626 deaths (9.7%), there were no pre‐existing conditions.’
‘In Scotland, 6.8% of deaths involving Covid‐19 from March to December 2020 had no pre‐existing conditions. In the same period, the Office for National Statistics found 12.5% and 17.2% of Covid‐19 deaths had no pre‐existing conditions in England and Wales respectively.’
‘The Health Protection Surveillance Centre in the Republic of Ireland found that those who died with confirmed Covid‐19 up to 12th December 2020, 93.4% reported an underlying medical condition. The differences in these proportions between countries could be due to differences in the methodology and demographic make‐up of each country.’
The definition employed by NISRA is that the ‘underlying cause of death’ is a ‘disease or injury which initiated the train of morbid events leading directly to death’. On its own Covid-19 causes few deaths yet the virus has assumed unprecedented power to freeze social activity and civil liberties.
All the factors that might cause the Irish State to have a better outcome have received little attention, including it having by far the lowest proportion of its population in the EU in the over 65s. As has been pointed out, 500,000 Irish people left for Britain in the 1950s and a further 300,000 in the 1960s. How many of these died in Britain who might have done so in Ireland?
There is no evidence that identifying those at risk and protecting them has been seriously considered or modelled. As I have noted in previous posts, the state has in fact failed these people in the guise of protecting everyone. That other states have also failed similarly has acted as some protection for them.
The issue isn’t that indoor hospitality has been postponed to whenever, or the unemployment or business failures that will result, or even that it has involved justification through discrimination. The issue is that it is yet one more example of an ‘abundance of caution’ ignoring the associated abundance of cost. Where is the modelling of the health and social cost of lockdown? Where is NPHET’s and the Irish State’s pessimistic ‘scenario’ for it?
