When University College Dublin virologist Dr Gerald Barry was interviewed by ‘The Irish Times’ and asked – why have we so many cases when we’re so highly boosted? – he said ‘Even asking the question points to the root of our problem in Ireland and in many parts of the world, we are using a tool that isn’t designed to stop infections and then wondering why it didn’t stop infections.’
‘I would strongly advocate for a complete reassessment of everything we have done to this point, identify everything else that could be done that would help, knock off everything that isn’t feasible or is unaffordable and do everything else.’
So we have failed? – ‘The problem with a “do more” strategy is that some countries that have demonstrably done less to curb the spread of infection, such as England, seem to be doing better overall.’
Just such a reassessment was recently reported in ‘The Guardian’ from Professor Mark Woolhouse, ‘one of the country’s leading epidemiologists’, who has written a forthcoming book, ‘The Year the World Went Mad: A Scientific Memoir’. Lockdown, he says, ‘was a lazy solution to a novel coronavirus epidemic, as well as a hugely damaging one”.
The day Britain went mad is reported as when ‘the No 10 briefing in March 2020, cabinet minister Michael Gove warned the virus did not discriminate. “Everyone is at risk,” he announced.’ To which Woodhouse responds: “I am afraid Gove’s statement was simply not true. In fact, this is a very discriminatory virus. Some people are much more at risk from it than others. People over 75 are an astonishing 10,000 times more at risk than those who are under 15.”
“We did serious harm to our children and young adults who were robbed of their education, jobs and normal existence, as well as suffering damage to their future prospects, while they were left to inherit a record-breaking mountain of public debt. All this to protect the NHS from a disease that is a far, far greater threat to the elderly, frail and infirm than to the young and healthy.”
“We were mesmerised by the once-in-a-century scale of the emergency and succeeded only in making a crisis even worse. In short, we panicked. This was an epidemic crying out for a precision public health approach and it got the opposite.”
That Covid-19 is a disease that discriminates is a point made often on this blog and by others, which should have signaled that a blanket approach wasn’t warranted. A recent paper analysing this has recently been published, which shows the disparity in effect by age, despite the difficulties in measurement.
It records that in ‘Twenty-five seroprevalence surveys representing 14 countries were included . . . the median IFR [Infection Fatality Rate] in community-dwelling elderly and elderly overall was 2.9% (range 0.2%-6.9%) and 4.9% (range 0.2%-16.8%) . . . IFR was higher with larger proportions of people >85 years. Younger age strata had low IFR values (median 0.0013%, 0.0088%, 0.021%, 0.042%, 0.14%, and 0.65%, at 0-19, 20-29, 30-39, 40-49, 50-59, and 60-69 years . . .’
These IFRs have been calculated using data from 2020 and are therefore before widespread vaccination, at least in richer countries and before the less virulent Omicron variant. We can therefore expect these numbers to have fallen not only due to vaccination but also better hospital treatment as lessons began to be learned about ventilation etc. The paper notes that ‘absolute risk values still have substantial uncertainty’ and mentions the low number of elderly in the studies examined by the paper, but which might also reflect uncertainty about the total number of infections and number of deaths actually caused by Covid as opposed to deaths of people with Covid.
The link here to IFRs for various diseases shows that for the younger age groups Covid-19 is far down the list. According to the European Centre for Disease Prevention and Control here Influenza (over all ages) appears more severe than Covid-19 for those aged below 30 although this also depends on the virus, host issues, and other factors.
The paper also notes that ‘besides age, comorbidities and lower functional status markedly affects COVID-19 death risk. Particularly elderly nursing home residents accounted for 30-70% of COVID-19 deaths in high-income countries in the first wave, despite comprising <1% of the population. IFR in nursing home residents has been estimated to be as high as 25%.’
Professor Woolhouse argues in ‘The Guardian‘ article that:
‘the country should have put far more effort into protecting the vulnerable. Well over 30,000 people died of Covid-19 in Britain’s care homes. On average, each home got an extra £250,000 from the government to protect against the virus . . . “Much more should have been spent on providing protection for care homes,”
He ‘castigates the government for offering nothing more than a letter telling those shielding elderly parents and other vulnerable individuals in their own homes to take precautions,’ something this bloggers’ wife found particularly galling as medical personalities and politicians congratulated themselves and were congratulated by others for efforts on her and others’ behalf which consisted of nothing much more than a letter.
As ‘The Guardian’ goes on in reporting Woodhouse’s views – ‘The nation could have spent several thousand pounds per household on provision of routine testing and in helping to implement Covid-safe measures for those shielding others and that would still have amounted to a small fraction of the £300bn we eventually spent on our pandemic response, he argues. Indeed, Woolhouse is particularly disdainful of the neglect of “shielders”, such as care home workers and informal carers. “These people stood between the vulnerable and the virus but, for most of 2020, they got minimal recognition and received no help.”
The British Government, according to Woodhouse, thus “lacked a convincing plan for adequately protecting the more vulnerable members of society, the elderly and those who are immuno-compromised.”
“Lockdowns aren’t a public health policy. They signify a failure of public health policy.”
The Irish State has reached the milestone of 5,000 deaths associated with Covid-19 at the same time as it controversially announced that there will not be a reopening of indoor hospitality on 5 July as planned.
Two weeks ago a government source had said that “the narrative that our reopening will slow down is not true.’ However that was before the National Public Health Emergency Team (NPHET) presented advice to it that a pessimistic ‘scenario’ forecasted 2,000 deaths over three months, largely due to the new Delta variant of the disease, with advice that only vaccinated people and those who have had Covid should be allowed inside restaurants etc.
Such a measure was denounced as ‘absolutely bananas” by one opposition leader amid accusations that it was unworkable, discriminatory and potentially illegal, never mind the damage to the social bond that arises from everyone making sacrifices together. Young people, it seemed, who predominantly serve in hospitality but are unvaccinated could serve, but not be served. Sinn Fein denounced the Government while more quietly accepting the decision; in this case talking more softly out of one corner of its mouth than the other. What would you do if faced with this dreaded forecast was the stock response from the governing parties.
While it was noted that NPHET had failed to factor into its assumptions newly allowed vaccination of younger people and there were calls for an independent audit of its modelling, plus claims that the Irish were an outlier in Europe in terms of indoor hospitality, by and large the figures were accepted without real challenge. The Irish State has had one of the strictest and longest lockdowns in Europe but if many more people are no longer so scared as they were, there is no alternative critical view of State policy beyond making it harder.
There are a number of reasons for this including that the Irish State has done relatively well in relation to deaths:
State support payments to the unemployed and businesses have continued, and political opposition, including from the left, has been in favour of even tighter restrictions. Such opposition as has declared itself, has been restricted to the far-right, including anti-Vaxxers who are easily dismissed but serve to make any other criticism easier to ignore.
The Irish economy is also set to grow by over 8%, according to the Central Bank, with this growth having less to do with base effects (the previous fall caused by lockdown making future growth easier statistically as well as economically) because the Irish economy has been hit less by Covid-19 despite the lockdown. The disproportionate presence of US multinationals, which includes companies in the pharmaceuticals, medical devices and IT sectors, has seen demand for their products increase.
An opinion poll in June reported that ‘fewer than one third of voters (32 per cent) agree that life should return “to the way it was before Covid” even after most people are vaccinated. Almost two-thirds (65 per cent) say that some precautions should remain in place, such as wearing masks in shops. Older voters remain significantly more cautious on this issue, with 79 per cent favouring continued precautions.’(Irish Times). The greater threat to older people goes a long way to explaining their particular concerns, as does the failure of the state to protect these people in its care or in private homes for which the state still has a responsibility.
That this number of people are so anxious is not a healthy sign, either from a psychological view or politically. A scared population is not one that is likely to be critical of state policy or seek to map out its own alternative. From a socialist viewpoint it is not conducive to independent thought by workers and rather affirms their social subordination. In this case the attendant denial of very basic civil liberties emphasises it.
Given the current very low level of cases, hospitalisation and deaths, plus the summer season, the dire warning by the Minister of Health, that “the biggest hurricane that has ever hit Ireland is coming’ simply reaffirms all these negative effects of state policy. Although one must assume his remark excludes An Gorta Mór.
The Government’s decision rests heavily on the most pessimistic of four scenarios presented by NPHET:
The presentation by NPHET shows a wide variation between a central scenario of 187,000 cases in three months and 545 deaths, and the pessimistic scenario of 682,000 cases and 2,170 deaths. Given the prevalence of the Delta variant, plus greater transmissibility by Alpha, it is the increase in social mixing that appears as the cause of the difference, but this is placing a big burden on indoor hospitality to make this the cause of such an increase. It is the possibility of the pessimistic scenario that is nevertheless given as the reason, although no probability is presented and the message appears to be that no possibility is acceptable.
The Chief Medical Officer has admitted that advice from his Scottish equivalent is that the Delta variant presents less risk of hospitalisation even if it is more transmissible. It is already well known that the virus is predominantly a threat to life to those who have other underlying health conditions.
The most recent figures published for the period up to 12 December 2020 report that 93.4% of deaths were of those with an underlying condition. The figures for those who had Covid-19 and also had an underlying condition was 16.9% for those aged 25 – 34, 52.58% for those aged between 65 and 74, and 59.4% of those 75+.
Clearly it is older people who are most at risk and it is mainly older people who are dying. The proportion of total deaths accounted for by 25 – 34 year-olds at 11 May 2021 was 0.81% while it was 15.5% for those aged 65 – 74, 33.75% for those aged 75 – 84, and 42.39% of those aged 85+. In other words, 91.64% of deaths were of those aged 65 and over, but being over this age is not sufficient to have a severe risk posed, you also need to have a relevant underlying condition.
NPHET has reported that cases amongst the eldest has fallen and lower than younger age groups, as this heat map shows:
This is due in good part to the vaccination programme prioritising by age but also by considerations of those most vulnerable. The programme has also prioritised health care staff although this was supposed to be targeted to front line workers. In the North not so much pretence was made and back-office support workers with no interaction with patients were vaccinated before, for example, immunosuppressed cancer patients. The mantra of ‘protect the NHS’ reached a logical conclusion when bureaucrats came before extremely vulnerable patients. While the Southern vaccination programme has been beset by some scandal in which relatives of senior executives and others favoured by them have been vaccinated out of priority, the existence of similar in the North has gone unreported.
In both jurisdictions the unchallenged requirement for vaccination of health care staff arises because both health systems have been incapable of implementing effective infection control. In part this is because of the large number of Covid patients hospitalised but this in turn has been mainly due to the failure to protect older people, including those in care and nursing homes. The Irish Government Covid-19 hub reported, as an example, that on Tuesday 11 May over half of hospitalised cases were in the over 65 age group.
In any case, the vaccination programme has gone a long way to protecting those most vulnerable. Among these the rates of full vaccination are very high – 94% of those aged 80 and over, and 91% of those aged 70 – 79. Among the 60 – 69 age group 43% are fully vaccinated while 93% have had one dose. Around 68 per cent of all adults have had one dose of the vaccine, while 45 per cent have had full vaccination. This compares with Scotland where the incidence of infection, and by the Delta variant, has dramatically increased but existing relaxation of restrictions, including on indoor hospitality, have remained.
However, the argument of the government and NPHET is that the vaccination programme has not progressed sufficiently to reduce the risk and that it is younger people who must be increasingly targeted by the vaccination programme.
However, it is openly acknowledged that the dire warnings and continued restrictions are based on uncertainty about the possible number of cases, the number that will be hospitalised and the number of deaths. NPHET has forecast 2,170 in the next three months in its pessimistic scenario, but this would mean an over 40 per cent increase in the existing death toll in a very short period, one-fifth the time of the preceding pandemic. This, when the most vulnerable have received some sort of vaccination, so protecting them to a significant extent against both hospitalisation and death, and against a dominant variant we are informed involves less risk of hospitalisation.
There is a final reason to be wary of attempts to frighten the population and potentially introduce discriminatory measures against those who face least risk. Leo Varadkar has written ‘that Ireland is among a small number of countries that includes in our numbers suspected and probable deaths from Covid even when the patient did not test positive or was not tested at all.’
The Northern Ireland Statistics Research Agency has reported that:
‘There were 1,626 deaths registered up to 31st December 2020 where Covid‐19 was identified as the underlying cause of death (88.8% of the 1,831 Covid‐19 related deaths). For 157 out of these 1,626 deaths (9.7%), there were no pre‐existing conditions.’
‘In Scotland, 6.8% of deaths involving Covid‐19 from March to December 2020 had no pre‐existing conditions. In the same period, the Office for National Statistics found 12.5% and 17.2% of Covid‐19 deaths had no pre‐existing conditions in England and Wales respectively.’
‘The Health Protection Surveillance Centre in the Republic of Ireland found that those who died with confirmed Covid‐19 up to 12th December 2020, 93.4% reported an underlying medical condition. The differences in these proportions between countries could be due to differences in the methodology and demographic make‐up of each country.’
The definition employed by NISRA is that the ‘underlying cause of death’ is a ‘disease or injury which initiated the train of morbid events leading directly to death’. On its own Covid-19 causes few deaths yet the virus has assumed unprecedented power to freeze social activity and civil liberties.
All the factors that might cause the Irish State to have a better outcome have received little attention, including it having by far the lowest proportion of its population in the EU in the over 65s. As has been pointed out, 500,000 Irish people left for Britain in the 1950s and a further 300,000 in the 1960s. How many of these died in Britain who might have done so in Ireland?
There is no evidence that identifying those at risk and protecting them has been seriously considered or modelled. As I have noted in previous posts, the state has in fact failed these people in the guise of protecting everyone. That other states have also failed similarly has acted as some protection for them.
The issue isn’t that indoor hospitality has been postponed to whenever, or the unemployment or business failures that will result, or even that it has involved justification through discrimination. The issue is that it is yet one more example of an ‘abundance of caution’ ignoring the associated abundance of cost. Where is the modelling of the health and social cost of lockdown? Where is NPHET’s and the Irish State’s pessimistic ‘scenario’ for it?
Following ‘the science’ and its scientists that we looked at in the two previous posts does not look well in hindsight, as a short review of the course of the pandemic in the Irish State demonstrates. In the early days these were forecasting 20,000 deaths, six times the current figure which is just over 3,300, and an even greater over-estimate than the influential Imperial College paper that forecast a possible 500,000 deaths in the UK.
At the start, what characterised the response, just like Britain, was complacency. On 4 March the Chief Medical Officer Tony Holohan of the HSE stated that “as things stand” there was no reason why the St Patricks day festival could not go ahead, and he did not believe that it was proportionate to prevent Italian rugby fans from visiting Dublin for a cancelled match. The attendance of thousands of Irish racegoers at the Cheltenham festival also went ahead. From the point of view of the generalised lockdown that was later to be implemented this was a catalogue of mistakes.
The State supposedly had a policy of test and trace, in which all cases could be identified and followed up to ensure isolation. The system and its resources were quickly shown to be inadequate, with it only subsequently being admitted that test and trace did not identify where infections came from. Prof. Philip Nolan from the National Public Health Emergency Team (NPHET) stated that “we would like to go back and find out where people are getting the virus, but we don’t have the time or resources to pursue this academic exercise”. In any case, in October researchers from Beaumont reported that up to two out of every three infections could be missed through poor technique when people are being swabbed.
At this early stage the policy on testing was confused: so to be tested before March 12 a person had to be symptomatic or either in close contact with a confirmed case or have travelled from an affected area. Then having one symptom was required, then the list of symptoms changed, and if this threshold was passed the person needed to be in a priority category.
These early mis-steps have led many to see the issue as being one of weak or incomplete implementation of policy rather than the policy being misconceived in the first place. The record suggests the latter.
The island of Ireland could not isolate itself from the rest of the world so could not avoid importing the infection. Having imported it, it was always going to be impossible to identify all cases since most were asymptomatic. Social distancing and isolation of suspected cases was considered to be the equivalent of the mass quarantine implemented elsewhere but was not. The measures adopted simply slowed the spread of the infection, justified to protect the health service, but with the by-product that doing so gave it time to mutate, as it did.
Much bigger ‘mis-steps’ were made at this time, again flowing not from failure to adequately implement policy but as a result of its conception. On March 6 the representative organisation of private nursing homes, Nursing Homes Ireland, (NHI) banned all visitors to its homes. Four days later Tony Holohan of the NPHET questioned the closures “before they are really necessary” while the Department of Health only eventually gave approval to the action ten days after NHI had introduced the restrictions.
In early March Holohan was claiming that ‘we had reacted very early and with significant action compared to other countries’, although the performance of these other countries seemed to be held up as some sort of exculpation rather than a pointer to a failing common approach. For the Chief Medical Officer their response “in the first instance had to focus on dealing with community transmission of this virus. There was simply no way of protecting nursing homes or any other institutional setting if we don’t control the spread of this infection in the community.”
NPHET later claimed that it was not until late March that research pointed to the threat of asymptomatic transmission in care homes although by the end of May Paul Reid, chief executive of the Health Service Executive (HSE), was acknowledging that “there are obvious gaps in clarity and responsibility in the overall governance and oversight of private nursing homes.”
By mid-April Holohan was stating that vulnerable groups in care settings were a priority, but by that time there were 330 outbreaks in residential cares facilities, with concern expressed about under-reporting. While boasting of the “unprecedented level of support” given to homes the HSE was unable to provide up-to-date figures for deaths.
Not much later Holohan was stating that it was “not realistic to think we could keep it out of homes”, while by the end of April it was reported that 735 people had died in residential community settings. By early May the mortality rate in nursing homes was three times that among the rest of population, accounting for 61 per cent of deaths (including those in other residential facilities).
By the end of May the Department of Health had been warned by the health regulator of more than 200 “high risk” nursing homes, while receiving “just an acknowledgement” and “no response”. NHI had quickly raised concerns around PPE and hospital discharges, but by late March 88 per cent of homes had bought either their own PPE or used home-made. Almost half of nursing homes said that they had to wait 10 days for test results to come back, and publication of cases in particular homes was not provided (unlike for hospitals).
By June it was apparent that nursing and other residential facilities were not the only health and social care facilities where infections were occurring. At the start of the month, it was reported that more than 200 people had contracted coronavirus while in hospital in 102 outbreaks. By the end of August, it was also reported that about 90 per cent of all cases among over-65s were of nursing home residents (between March and end of June), amounting to almost 6,000 cases resulting in 968 deaths (56% of the total at that point).
By the beginning of the following month concern was again being expressed at the rise in cases among older people. In early October a NPHET letter noted a ‘sustained increase’ in cases, with home residents accounting for more than half of the 1,810 virus-related deaths, but with Holohan again asserting that it was not possible to document all patterns of infection and that measures directed to the whole population were needed.
The Health Information and Quality Authority (HIQA) expressed concern that there was no “consistency of approach” on whether nursing home residents should be tested where staff had tested positive. The HSE chief clinical advisor claimed that older people could not be “siphoned off safely” but the chief inspector of HIQA stated later that “not all centres where staff have tested positive have undertaken a programme of resident testing.”
In November, NPHET priorities, according to Holohan, were protection of the most vulnerable, continued resumption of non-Covid health and social care services and education of children; but by mid-November it was reported that in the week up to Oct 31 there were 56 outbreaks of infection in nursing homes and 33 associated with hospitals.
Lockdown however appeared to be getting some results, even if this was little more than postponement rather than eradication. This was now success, as was the perceived protection of a health system unable to adequately do its own job of protection.
By the beginning of December the Irish state was hailed, especially by itself, as the best performing in Europe measured by the average number of new cases. Unfortunately, even in success the most significant threat remained, with Holohan expressing concern at the level of infections in nursing homes despite the highest Level 5 lockdown. Hospitals also remained a problem, and on 13 November it was reported that pre-admission tests for Covid that had been recommended for hospitals were not being practised by all. Anne O’Connor, the chief operations officer of HSE, stated that guidance had been changed in the previous two weeks.
By December the problem with hospital acquired infection was continuing, with over 200 confirmed cases in the four weeks up to 13 December and more than 400 picking it up in hospital in two weeks in January. By the new year the Irish State had gone from the being the best in Europe to being the worst in the world in terms of growth in cases. The State went from 80,000 cases in nine months to doubling this total in three weeks.
Since there had been a partial opening before Christmas this was held up for blame but there remained no evidence that cafes, hairdressers or clothes’ shops were a problem; it was a question of a seasonal infection flourishing in its best environment with any human interaction facilitating spread.
Doing away with the latter altogether was the only logical extension of the existing policy and all the variations on the different social distancing rules were the proverbial number of angels dancing on the head of a pin. Very few wanted to go there, and those who might would face the difficulty that closing down sites of infection might have to start with hospitals and nursing homes, with 100 outbreaks in the former from July to mid-December and 93 in the latter. A study in mid-January reported that the rate of infection among hospital staff in Galway and Dublin was six times that of the local community.
Despite the months of restrictions and despite the worst-in-the-world figures there did not appear to be excess deaths. The prevailing narrative appeared to tell a story that did not add up. One aspect however appeared stubbornly consistent, the median age of those dying was reported in mid-January to be 82. This outcome was consistent with the North despite its apparent different path, with people aged 75 and over accounted for 77.7 per cent of ‘coronavirus-related’ deaths and with 91.5 per cent having some pre-existing condition, Dementia and Alzheimer’s disease being the most common.
On 20 April last year the lead story in ‘The Irish Times’ was a report of research led by an Irish scientist that there may have to be repeated waves of Covid-19 epidemics until enough of the population is infected to provide herd immunity. At best there would be three more infection cycles before 60 per cent was infected, enough for immunity.
It reported intense debate on the subject, with World Health Organisation epidemiologists warning that there was no proof yet that having the infection would confer immunity for a significant period of time. Later, when it was apparent that immunity did occur, the response was that the level of antibodies recorded in previously infected cases declined more or less rapidly so that immunity would also decline. This however did not take account of the body’s reduced need for higher levels and its newly acquired capacity to ramp up again if required; it also did not take account of the role of T-cells in fighting infection.
The point however, is that herd immunity was not dismissed as beyond the pale and was not considered a euphemism for mass murder. In fact, as the link to the debate below records, herd immunity is not so much a strategy as an outcome, the inevitable outcome of defeating the pandemic. That it has been understood as anything else illustrates the impairment of critical thought that has accompanied the physical restrictions introduced by lockdown.
Throughout the pandemic, governments in Ireland, Britain and elsewhere have been keen to demand that people follow ‘the science’ (as they put it), backed up by certain scientists or doctors, usually on the state payroll, who have given authority to government policy even when it is sometimes reported that they don’t agree with it.
The appeal to authority, the idea that there is one ‘science’ with one rational direction available to policy makers, the unwillingness to debate, and repeated charges of lack of transparency; all these are very far from any scientific approach. The debate here on what the correct approach should be is an example of what has not been presented to populations. The effects of this have been many and not always acknowledged.
I recently had a disagreement on Facebook with a supporter of a ‘Zero-Covid’ strategy, who refused to accept our differences were political, claiming that there was a psychological issue involved with my approach (along with some other remarks I have committed to amnesia). The alternative that I argued, of focused protection of the vulnerable and opposition to generalised lockdown, was not received as a legitimate one to be considered, but simply one to be condemned and damned as so mistaken as to be the product of some psychological imperfection.
What was remarkable was that the principal issue facing the world was argued as something above, beyond or otherwise disassociated from politics. Marxists, and this guy is one of long standing, are supposed to base their ideas on the reality that science, morality and all aspects of human behaviour are permeated with politics. Science has its political aspects and the actions of the Government and state obviously does, especially when they involve drastic restrictions on human activity.
So, to regard Covid-19 as a non-political issue is absurd. That such an argument could arise on social media is not at all surprising since everything under the sun appears on it. In this case however the response is not uncommon, and is a mirror reflection of the approach taken by almost all Governments, which is to deny legitimacy to any questioning of their policies. We can see this clearly for example in the pathetic ‘opposition’ of Keir Starmer, whose only point of disagreement is that the lockdown policy of the Government has been implemented incompetently and incompletely.
The policy of inducing fear into the population is ably assisted by a willing media seeking the simple and the sensational, through stressing the lethal nature of the virus; repetition of statistics on cases, hospitalisation numbers and patients in intensive care; the numbers with ‘long-Covid’; the prominence given to sufferers among the young, and of course the rising number of deaths.
This goes along with a determined policy of down-playing the specificity of those most under threat, and claims that the virus is either out of control or will utterly swamp the health service. The fear generated has enough truth behind it to get acceptance of actions that would in normal times have generated heated opposition; including cancelled urgent cancer operations and a policy of isolation of individuals that admits that increased domestic abuse and enormous deterioration in mental health will follow. The cumulative effect in generating fear is to dampen and discourage further the exercise of people’s critical faculties.
Instead of opposing all this, much of the left has echoed it and amplified it, as my minor Facebook argument illustrated. This Left demands stricter and longer lockdowns and ‘zero-Covid’, i.e. no cases and no deaths from Covid. To state that there is an alternative approach to generalised lockdown, and admit that some deaths will almost certainly result, is to damn oneself out of one’s own mouth. How dare you advocate a policy that accepts any deaths!
We will, for the moment, leave aside the obvious truth that the current lockdown policy has abysmally failed to prevent avoidable deaths, and that the ‘Zero-Covid’ policy has yet to indicate what injury and deaths would flow from its implementation. It has failed to admit that it would have to be enforced; that the state would have to do the enforcing and that it would have to apply much enhanced powers of coercion to attempt to achieve it. An additional result would be to limit further the space for open debate on different approaches and alternative futures following the pandemic.
The policy of the Left has not been to encourage scientific debate but to back one element of the consensus view that lockdowns are the answer. The problem here is that there has been far from a free debate on what the best approach to dealing with Covid-19 is and not, as the left would have it, a refusal to follow through on what is so obviously the right, or rather only, one.
These two articles, here and here, show that there is no single and unequivocal scientific approach that supports lockdown. Rather, there is an intensely political debate within the scientific community that has suffered from, but resisted, restrictions on discussion. The result of the attempt to impose a single approach has been the development of what has been called ‘groupthink’, censorship and self-censorship and something of a climate of fear, in which critical thought is seen as criticism of the scientific establishment, which might be damaging to the careers of those who engage in it.
The inevitable uncertainties generated by a new viral infection requires engagement with the issues that the political establishment does not believe the population can handle, something the media reinforces with its superficial treatment of every issue. The mechanisms and apparatus that circumscribes political argument has been easily employed to narrow debate on the right approach to dealing with the pandemic. The idea that the issues around it are non-political is, to repeat, ludicrous.
This political debate has been grossly distorted by an anti-scientific assault by the far-right, typified by the often-imbecilic antics of Donald Trump, with his alternative denial of the virus, its importance, his success in dealing with it, and his recommendation about drinking bleach. The mass base of scientific ignorance he mobilised in the US has been reflected everywhere to a greater or lesser extent. The effect on rational criticism of the prevalent lockdown approach has been to prejudice reception of it and create a barrier to its discussion. Sections of the left have joined in, unwittingly contributing to the anti-scientific shut-down of rational debate. As with so many issues, the opposition to lockdown by sections of the right, whether of the crazed anti-vaxxers or libertarian conservatives, has been the cue for some on the left to take an opposing view.
We are over a year into the pandemic, about a year since it hit Europe, and there is no excuse for lack of debate on how to deal with it. Only episodically has one taken place in Ireland and like everywhere else, any alternative to lockdown has been subject to condemnation. It has had its own share of far-right sceptics that have made the task of challenging the lockdown consensus harder; but the fact is that the policy of lockdown has failed, and the experience of the last year has proved it, which is what we will review in the next post.
The policy of lockdowns has been approved by many on the left, with the additional argument that they have not been strict enough. Some appear to believe that pandemic induced crises necessarily open up opportunities for revolutionary crises. These are considered opportunities to mobilise the working class to resist attacks on its social position and turn it towards socialism. Crises then become both the necessary and sufficient condition for political revolution. What these sufficient and necessary conditions might actually be is not considered. That question has been answered and is no longer a question.
Previous crises have not entailed socialist revolution, but rather than investigate why this is, the approach has been to lament the weakness of the revolutionary left and the treacherousness of existing working class leaders. Crises therefore are expected to do much of the heavy lifting of working-class political consciousness, allied to an unexplained rise to prominence of revolutionary organisations. Rather than see such crises as occasions of potential radicalisation which must be based on prior conditions giving rise to class consciousness, this consciousness is assumed to arise from crises itself and the spontaneous activity generated. This latter activity is then fed by Left economic and political demands that further radicalises it.
This process however requires prior development of the working class, including organisation and consciousness which already disposes the working class to defend itself through ‘spontaneous’ mobilisation that rests on some prior socialist consciousness. We know that a lack of such consciousness has not been overcome by crisis in itself because of previous decades of defeats of working-class struggle; from a sober assessment of current working-class consciousness and passivity, and from appreciation that the last real revolutionary period rested on this prior development of socialist organisation. Of course, many struggles in this period were betrayed by reformist and Stalinist leaderships but these betrayals had precisely the effect of setting the working-class back decades. It’s why continuing opposition to these political trends in the working-class movement is a continuing imperative. But it is wrong to simply repeat the explanations of previous defeats that happened decades ago as applicable now to much later generations.
In demanding a more stringent lockdown the purveyors of this general view rally behind the most lurid and sensational predictions of the effects and deaths that will be caused by Covid. The pandemic itself has become a ruling class conspiracy – “as far as the ruling elite is concerned, if the old and infirm die and allow for further cuts to pensions and health care, that is to be regarded as a positive good.” As has been pointed out: across the world capitalist governments have spent fortunes in response to the pandemic. If their objective has been to save money they have failed abysmally. In Ireland and UK the state has borrowed billions and seen their debt mushroom as a result.
If their favoured policy of total lockdown requires emulation of the approach of China, Australia and New Zealand etc., as some have claimed, then why are these countries not also in on the conspiracy?
This left appears oblivious to the cost of lockdown in terms of deaths, illness and social and economic loss; and sliding over who suffers these costs: from the lost jobs, education, domestic violence and damage to menial health. It may point to the massive and wasted expenditures on testing and tracing systems that don’t work, and from failed and corrupt contract awards for PPE etc., but what has facilitated this?
They don’t stop to consider how their approach supports the politicians and state bureaucrats who cancel cancer and other life-saving treatments in order to protect their politicised health choices, and a health system that is failing and for which these politicians and bureaucrats bear responsibility. Instead, their demand for lockdown puts the onus on the population to accept the most restrictive forms of social control and denial of civil rights, opposition to which is another one of their conspicuous silences.
Instead they oppose the opening of schools, though children are not at significant risk and infections in schools are low (see here and here and here). One organisation dismisses schools as a “child-minding service’ employed to force parents into work, oblivious to this being a service that many parents are very glad of. It complains of trillions going to corporations but ignores that this is a product of lockdown; or do they believe that the state would give money to furloughed workers and not corporations? What would happen if they didn’t, would all these corporations survive?
This organisation proposes committees that “would provide the means to organize a Europe-wide general strike to compel the closure of schools and nonessential production and allow workers to shelter at home.” A stay away from work in order to get paid to stay away from work! Since when did the capitalist class pay for an indefinite general strike? And how would one be organised with the mass of workers at home and socially distancing? How would any revolutionary potential of a general strike be realised, i.e. acknowledging that society cannot simply close down but must continue to run, raising the question of who runs the economy – who rules? How would this be possible unless major sections of the working class were actually at work?
“Massive resources must be invested to provide a high standard of living to everyone throughout the pandemic, including the resources required to maintain online learning for students.” But how could anything be invested if the workers required to deliver the investment are to stay at home? Or is this yet another essential section of the working class that must work – like so many the total-lockdown supporters refuse to acknowledge.
“The claim that there is “no money” for such measures is a patent lie. Trillions of euros have been handed to the banks and corporations in bailouts since the beginning of the pandemic. The resources exist, but they are monopolized by a corporate and financial oligarchy.” The utterly un-Marxist idea is again advanced that money can equal “resources” and that pieces of paper are of use without human labour to deliver the real goods and services for which they are exchanged. And anyway, isn’t the monopolisation of productive resources by a separate class not called capitalism?
Indeed it is, which once again demonstrates that every intervention by the ultra-left telescopes into demanding the overthrow of capitalism.
“The fortunes of the rich must be expropriated and the major corporations transformed into public utilities, democratically controlled by the working class as part of the socialist reorganization of economic life on the basis of social need, not private profit.” But how are “the major corporations” to be put under the control of the workers unless they are actually at work?
As we know, Covid-19 is a specific threat that must be defended against. When advocates of total lockdown call young people having a party ‘granny killers’ they acknowledge this reality. Yet the pretence is still made that everyone is equally threatened at least to such degree that no strategy must distinguish between those who are old and/or otherwise vulnerable and those who are relatively young and healthy. Students must go home, schools must close and young people socialising is an existential threat.
What this does is weaken the protection of those most at risk because it calls into question any restrictions. If there really was no significant differential impact then many thousands of young people would have died. They haven’t. Many working class people, as I have noted in previous posts, and here in a previous comment by a reader, are ignoring the rules when it suits. The left advocates of complete lockdown are really now following Bertolt Brecht when he said – should this left not just elect a new people?
Most people however do register the greater threat to older and vulnerable people but rather than this being informed, encouraged and organised it has more or less been ignored by the authorities when it comes to organisation of the response. Tightening restrictions affects everyone, and in some ways young people more, and undifferentiated relaxation exposes older people more because it cannot be admitted that they should still be shielded or socially distanced; just in case everyone decides that is the way it should stay, that this is the correct approach that should now be implemented and those in charge have got it wrong.
This approach has failed in Ireland, Britain and across Europe and further afield. Part of the left doubles down and says the lockdown is not tough enough, without weighing up the cost or admitting that total lockdown has never actually been implemented because it can’t. You cannot close down society, which relies on the continuous labour of millions of workers. Admission that ‘essential’ work must continue never admits the enormous extent of what this entails given the development of the forces of production and division of labour involved.
A blanket threat in many ways protects the authorities from blame for failure because Covid-19 becomes an all-embracing indiscriminate threat that is difficult to defend against because of this character. It allows them to introduce harsh social restrictions and coercive powers that for most people are totally unnecessary, and which some on the left who, were they consistent, should support because (1) they should endorse a fair claim to be necessary and (2) totally warranted given the assumed threat. What could be more important that saving lives?
The longer the pandemic lasts the more incredible become the demands for total lockdown and ‘zero-Covid’. The failure of existing restrictions has been too great to inspire notions that just more of the same will be both successful and at an acceptable cost. Given the attacks stored up for the future, there will be plenty of time to reflect on the lessons.
The Northern Ireland Health minister was interviewed on the BBC here. After first saying that he didn’t want anyone in the health service to be put in a position of making ethical decisions to deny essential medical treatment the interviewer told him that the Chief Executive of the Belfast Health Service Trust has said that they are already being made, and are life and death decisions. Does Swann deny this or say he will investigate? No. He immediately and without hesitation attempts to justify something he said he didn’t want to happen, as if it hadn’t been happening.
He says that these decisions have to be made – “the ethical decision is could we turn a Covid patient away? The answer is no.” For other patients, “sorry your operation, your scope your diagnosis is going to have to be put off.”
When it is put to him that what he is saying is that a Covid patient won’t be turned away but that the result of this is that a cancer patient may die his answer is “yes, that’s as black and white as it is.”
So how is this ‘black and white’? There has been no medical assessment provided that this blanket prioritisation is justified, in fact it is presented as if its justification is self-evident, an obvious ethical decision. Except it’s not obvious and it is without justification, in both senses of that term – it has not been justified and any attempt to justify it would be wrong.
Swann says that we ‘cannot turn a Covid patient away’ but we already know that while over 50,000 people in the UK and over 3,000 in Ireland have died with Covid it is not at all clear how many of these have died of Covid. So how can this particular disease be prioritised?
More people die of cancer than Covid-19. There are around 165,000 deaths from cancer in the UK – that’s every year. In 2018 over 4,000 people died of cancer in Northern Ireland. In the Irish state over 9,000 die every year.
It cannot be because of the severity of the disease: cancer kills cancer patients because of their condition, while for most sufferers of Covid the disease is so mild they may not even know that they have had it. If someone with Covid has a serious underlying condition making them vulnerable to death compared to a relatively healthy person with the same disease, what is it that makes the difference between survival and death? Covid may be the proximate cause of death but Covid may not be the underlying condition without which death would not occur. If this is not considered an important distinction then presumably the health service and whole swathes of the economy will close down during the next flu season. A report from the Health Information Quality and Quality Authority shows that not all ‘Covid deaths’ should really be counted as such (see below).*
There is little that can be done to avoid many cancers; even those who don’t smoke, eat healthily and exercise fall prey to it. Hospital treatment is necessary but can sometimes require less serious intervention if caught earlier, although this is precisely what is being deprioritised. Those most vulnerable to Covid on the other hand can take many of the measures we have all become accustomed to including social distancing etc. The most vulnerable received shielding letters informing them of their vulnerability and measures they might want to take to limit exposure to infection. Swann and his chief medical advisor have decided that these letters aren’t necessary this time but provided no real explanation why. What has changed from the first lockdown?
Why is the protection of those most likely to suffer fatalities from Covid not the major focus of protection, support and prevention from these political leaders and bureaucrats? Is it not really that, what both measures have in common – prioritisation of Covid patients within hospital and lack of focus on those most vulnerable – and what is being protected, as they have made clear repeatedly, is the NHS? Protected from doing a job they know it will fail? And by their association, responsibility and accountability for it, protection of themselves?
The NHS in the North of Ireland is the worst in the UK. There are, for example, more than 2,500 nursing vacancies. As I have said before, Covid-19 may overwhelm the resources of the health service but is in itself not overwhelming. It is only so because the NHS is already in crisis, and what we are asked to do is also to accept that we must collude in covering up this permanent crisis, including through regular speeches telling us how difficult it has been for the staff.
This message is all the more powerful, and successful, because it is largely true – many health service staff have been under enormous strain but this should not be an alibi for failure of the bureaucracy that is the NHS as an organisation. As I have said before, the demand to protect the NHS, when it is supposed to be there to protect us, is an admission that this responsibility of the NHS will not be met.
The unjustified blanket prioritisation of Covid patients in hospital and the failure to issue shielding letters to the vulnerable are political decisions and have been successful because of a political campaign to justify lockdowns. This has involved not only politicians but also senior health figures, who have given legitimacy to their decisions. One such figure has been Gabriel Scally who has regularly intervened to argue that policies in the North and the South should be the same, as if two wrongs make a right. He has stated that ‘the figures speak for themselves’ when it is well know that they don’t, and has stated that over 50,000 have died of the disease without recognition that dying with it is not the same as dying of it. That such basic errors are repeated by a respected public health doctor illustrates the scope of the group think that has developed.
So egregious was the Health minister’s statement that the Department of Health put out a tweet entitled ‘Myth Buster’ with ‘myth number 1′ being “are Covid-19 patients being prioritised over other patients?” To which the answer was “No, they are not. Patients are treated according to clinical priority.” Swann pitched in with “it is untrue and offensive for anyone to accuse frontline staff of prioritising one condition over another.”
Since it was Swann who said that prioritising was ‘black and white’ perhaps it is himself he is referring to as being offensive. So who is right – the Department or the minister, and which version of the minister?
It would be difficult to deny that senior health staff would not be so stupid to as to admit such crass medical practice but easy to understand how Stormont politicians could grandstand with this level of idiocy and ineptitude.
The real problem is not that some politician has instructed hospital doctors to relegate individual cancer patients in order to prioritise Covid patients but that this is what has and will continue to happen by political decisions on allocation of resources that constrain individual medical assessments. These individual decisions rely on higher level decisions on allocation of staff, wards and beds to deal with Covid that in the first wave witnessed empty Covid beds in the Nightingale hospital while other treatments were stopped.
Lockdown is a political decision involving an analysis not only of the disease but the potential impact of the response. It is not a question of medical expertise determining the correct approach, even if one were naïve enough to believe that the medical profession is a paragon of virtue and wisdom. The advocates of lockdown refer regularly to the number of cases, hospitalisation cases, numbers in ICU and deaths but rarely to the costs incurred by lockdown. To do so would invite a critical debate they are ill prepared to have. Swann’s mistake was to take soundbites to their logical conclusion and blurt it out. It denotes the logic of the current approach but too crudely expresses its effects.
It is tempting to see in Swann’s first statement the chaos and breakdown of the functioning of the Stormont Executive that because of its reaction to the pandemic was seen for a while as an example of the political arrangements working. No one is pretending they’re working now. However, the real political weakness lies not in the political primitiveness of Stormont but that such crass political interventions elicit no popular opposition. Unfortunately on this score looking for the left to offer one would be a complete waste of time, as we shall look at in the next post.
* HIQA: ‘The officially reported COVID-19 deaths may overestimate the true burden of excess mortality specifically caused by COVID-19. This may be due to the likely inclusion within official COVID-19 figures of people who were known to be infected with SARS-CoV-2 (coronavirus) at the time of death who were at or close to end-of–life independently of COVID-19 or whose cause of death may have been predominantly due to other factors.’
The advice from the health experts of the National Public Health Emergency Team (NPHET) was that it was necessary to move from level 2/3 to level 5 because this was the “only opportunity” to get Covid-19 “back under control”. But when this was rejected by the government and Leo Varadkar went on TV to cut the Chief Medical Officer (CMO) off at the knees, he damned not only the CMO and his advice but also the strategy of his Government.
Not only could it no longer be claimed that government strategy was the product of expert advice, but it raised the obvious question why total lockdown was previously implemented. If it was necessary in March there was no reason it wasn’t necessary now. Where is the improvement in the test and trace system and health service capacity over the summer that might have been presented as some sort of explanation for a more relaxed policy now?
All the questions raised in my previous post could be asked again, including how the different levels of intervention make any sense when, for example, the criteria that are supposed to prompt intervention are the same for levels 2 to 4. In the previous post the question was where was level 2 and a half, or 3 and a bit, applied to Dublin? Now it is – what are all these levels for in the first place?
There are of course real concerns, such as the reported “sustained increase” in cases among the elderly with seven new outbreaks in nursing homes in the previous week, especially when we recall that over half the deaths have come from these facilities. But this too raises a question – if lockdown didn’t prevent these deaths then, what would lead us to believe it would do so now? After all, we have been told that to protect the vulnerable we have to have complete lockdown but it didn’t work before – why not?
And if the NPHET is the while knight alternative to the Government – where have the warnings been about the preparedness of the health service and the vulnerability of the old and special measures proposed to protect them?
Instead we have a lower level of restrictions, although still based on the same assumption that everyone must be isolated in order to also protect the vulnerable. To present a show of real intent thousands of Garda, at hundreds of road blocks, have attempted to prevent the whole population from moving outside their county (as if these were epidemiologically significant boundaries) in order to deliberately gum up traffic, when such movement is entirely legal.
Apparently Varadkar had some tough questions for CMO Tony Holohan, like what was the metric for success and how long would the lockdown last? There has even been speculation of following the widely trailed policy supposedly to be implemented in the North – a ‘circuit breaker’, i.e. a relatively short lockdown to bring the virus ‘back under control’. But this can’t explain why a shorter repeat of the last lockdown will not result in the same increase in the virus when it ends.
Unless, of course, as I noted in the last post, the spread of Covid is much greater than reported, in which case the rationale for lockdown is even more undermined.
Varadkar also apparently said to the Chief Medical Officer that Ireland needed a plan in case this one didn’t work and a plan for re-opening if it does, and a plan for communications as well. A bit rich coming from Varadkar you might think, since if we work our way backwards on this list, the Government screws up communications each time it attempts to communicate; a plan for re-opening should already be in place since we have already had a re-opening; and we should also have a plan from the Government if lockdown doesn’t work since we have had a lockdown and it didn’t work.
Which neatly brings us to the need for an alternative. As in the previous post, we can briefly review what has been proposed by some of the left, by People before Profit (PbP), which has beefed up its press statements and explained a little more about its zero-Covid policy. This it seems “does not mean we reach absolute zero in terms of cases. It means crushing the virus to the point where we can test, trace and isolate every single case that arises, stopping the spread of the virus.”
But if up to 30% of positive cases show up as negative then it is impossible to “test, trace and isolate every single case.” Never mind the prior problem that, as The Guardian newspaper reports, “researchers at UCL said 86.1% of infected people picked up by the Office for National Statistics Covid-19 survey between April and June had none of the main symptoms of the illness, namely a cough, or a fever, or a loss of taste or smell the day they had the test. Three quarters who tested positive had no notable symptoms at all.”
The proposals by PbP support level 5 lockdown and include expansion of testing and tracing and health services; increased workplace inspections and more money spent on teachers with the potential for closure of schools “until the virus is crushed.” Inexplicably, there is no specific mention of those most at risk. Nothing is said about how long this lockdown would have to last and what the financial cost would be. Nothing, in other words, about the deaths and illness caused by prolonged isolation, a health service diverted from its day job or the long-term effects of a prolonged lockdown.
There is also nothing on the level of State coercion that would be required to impose a more severe lockdown with an indefinite timescale. People before Profit is kidding itself if it believes that this would not be required.
It calls for a harmonised response across the island but the problem isn’t harmonisation, it’s that both jurisdictions are making the same mistakes. To little public response the Health Minister in the North reported that there was, after all, to be no announcement on plans for the NHS to return to normal operation – how and when it will return to delivering all the health and social care that consume more lives but are not now so politically prominent. There was a time when Sinn Fein complained of political policing, but now it is in office we have the previously undreamed problem of political health care.
The Guardian has another article ‘Why herd immunity strategy is regarded as fringe viewpoint’ that criticises a strategy focused on protecting the most vulnerable, those at most risk. Unfortunately it ignores the failure of the current strategy in Britain, which is due not simply to Tory mendacity and incompetence.
The alternative is damned for being outside the ‘scientific mainstream’ and having extreme right-wing supporters, neither of which proves anything more than these bald facts. It quotes one professor who ‘is among many scientists who are sceptical that the most vulnerable in society can be adequately identified and protected. “It is a very bad idea,” he said. “We saw that even with intensive lockdowns in place, there was a huge excess death toll, with the elderly bearing the brunt of that.” In the UK, about a quarter of the population would be classed as vulnerable to Covid-19.”
This is stated almost as if 25% is too great a number to protect. So let’s go for 100%? They can’t be adequately identified and protected? So why can’t the health service and social services be mobilised to identify them from its records and then put in place measures to support and protect them? Why would it be a problem, for example, to identify everyone in elderly person’s homes? Or receiving treatment for those underlying conditions that make them vulnerable? Even the first measure might have made a major contribution to protecting half of people who died but were supposedly being protected by measures aimed at everyone else.
And let’s not forget that primary among that to be protected was the health service itself. As I’ve pointed out before – isn’t it supposed to protect us?
Another biostatistician is quoted as saying that actually this strategy of protecting the vulnerable was tried – “Shielding of the vulnerable was part of the UK policy since the start of lockdown.” Except of course, this was never true, not in Britain and not in Ireland either, as the irresponsible transfer of the elderly out of hospital and into homes with their lack of PPE testing and adequate staffing amply demonstrated. To claim otherwise is to admit the existing strategy had to entail these deaths – not something you will hear or read very often.
“What troubles many scientists is that with coronavirus no one knows how protected people are after contracting the virus, how long that protection lasts, and exactly what proportion of society needs to be immune to quell a pandemic.” All good questions, none of which provide support for the existing strategy or damn the alternative; or address the fact that the relatively young and those without the relevant underlying conditions have little to worry about. These concerns apply equally to a vaccine, but no one will advance them as objections to vaccination.
“It is impossible to fully identify who is vulnerable and it is not possible to fully protect them.” But is it harder to protect them than to fully protect everyone?
‘Another concern many scientists raise is the impact on the young and healthy. While the risk of death is low in people under 40, infection can still expose them to long-term complications that healthcare could be left dealing with for decades . . . “Quite large numbers of younger people are already becoming infected at present, whether or not they are being encouraged, and there are consequences to those infections.”
There do indeed seem to be some consequences for some younger people but transparency on this, how many there are and what the effects are, is not readily available. But it is not possible to put this into perspective with a strategy that is based on treating the whole population as if it was under the same threat. Identifying exactly who is at risk and of what is not what the current approach is about, and scare stories and sensationalist reporting are instead the order of the day.
If socialism is about building a counter-power within capitalism that fights for its replacement this must include the development of the organisation and consciousness of the working class, starting with its labour movement. This organisation must include scientific bodies and scientific consciousness. We don’t have working class scientific organisations – bodies consisting of scientific professionals belonging to or sympathetic to the labour movement or socialism – but the Covid-19 pandemic is one more lesson that we cannot afford to accept that the state, in its welfare guise or not, will provide the protection or support we need.
Beyond the arguments over the failure of almost all capitalist states to protect its most vulnerable, and the strategies that would most successfully address this need, lies this longer term task that the labour movement and socialists must accept and seek to address now and after the pandemic is over.
Just over a month ago my wife and I visited my daughter, her boyfriend, and my sister in Glasgow and had dinner in my sister’s house. Two weeks later this would not have been possible, I would have been breaking the Covid regulations; in fact, my daughter and sister couldn’t have done it together even without us. They could, however, have met together in the pub, which of course doesn’t make much sense, as this Scottish blogger argued.
This week new restrictions were introduced in the North of Ireland, and even more stringent ones in Belfast and a number of other areas, making breaking of the regulations inevitable. This has led to the targeting of students returning to University and partying in the Holyland area. As some students have pointed out – we can’t party in numbers in our houses or on the street but we can all go to the Hatfield bar and ‘socially distance’.
When more restrictions were to be introduced by the Government in Dublin it was also stated that it would be looking at opening ‘wet’ pubs (that don’t serve food). Later it suffered complete derision by asking publicans to keep receipts showing that punters had indeed ordered a panini costing at least €9 when they had bought their pint of Guinness.
This week it unveiled a new strategy that had five levels of restrictions, leaving Dublin to fall into level two and a half! The Health Minister took sick on the day of the launch and had to isolate, causing the rest of Cabinet to briefly join him. Since all these rules and regulations are based on assigning individual responsibility for avoiding the virus it wasn’t a good look.
In all these jurisdictions the number six has become a new guideline for people meeting up, the number to be made up – or not made up – of children and belonging to one, two or three households, sometimes differing between indoors and outdoors. Overall however the differences seem less and less important.
The timing and severity of lockdown has proved no protection as infection rates increase in Dublin, Belfast and Glasgow while various parts of England are subject to greater restrictions every week. In all places the threats of a second wave reveal the failure of the measures to deal with the first, and in all of them, despite its much-vaunted role, the test and trace systems are not operating as the should. The readiness of the health services is unclear, but only in so far as the extent of new wave of infection is unclear, otherwise the inadequacies of each health service is perfectly clear.
Such inadequacies were the subject of a column in the Belfast paper ‘The Irish News’, in which was noted the absence of protest at the local NHS having almost closed down. The lockdown has led to much reduced access and reduced capacity, on top of waiting lists much worse than those in Britain. It has been justified in terms of keeping Covid out of hospitals and preparing for the second wave but deaths have now arisen in two hospitals – so it isn’t working. In the South, the number of people screened for cancer was down 60 per cent in the first six months of 2020 compared to the previous year and the already unprecedented waiting lists have increased.
The so-called second wave was to be addressed by much improved test and tracing systems. Unfortunately, the system in England is reported to be collapsing and the Irish one is nowhere near what was projected as necessary in April. While still considering itself better than the British, the Irish are testing 1.8 per thousand people while the UK is doing 2.43, and has been achieving this only by using scarce heath care staff to do the testing, meaning they can’t do their day job. In Scotland pressure on the system has meant results are taking up to ten days to come through with this reported to be threatening the regime for care workers in elderly persons’ homes.
In all countries extra funding for health services have been announced as if this will quickly address the neglect and austerity these services have suffered for years. The additional funds are a reiteration, on a much greater scale, of repeated funding for new initiatives that are periodically announced but that rely on recruiting health professionals from other parts of the service, which create problems further back. It’s as if you can deploy thousands of trained medical, nursing and other professional staff in a matter of weeks or months despite taking years to train them and years to put in place new facilities for them to work in.
The announcement of potential fines of £10,000 in England is many things, but an effective public health measure it is not. It will discourage compliance with the rules and disaffection with the whole public health campaign. The call for respect for the law, given the exclusion of Dominic Cummings from its requirements and the threat to break international law over the Brexit Withdrawal Agreement, is too obviously hypocritical to be acceptable. The result will be intensification of blame on the general population for the Government’s failures.
Irish public health officials have warned of an increase in cases in the over-75s, the most vulnerable group and those who have suffered the greatest loss. The argument advanced is that the whole population must suffer increasingly arbitrary and unenforceable rules to protect its most vulnerable section. But all this achieves is failure to focus on targeted measures that might work in protecting the vulnerable, through steps to support their social distancing, ensure safe care home environments and safe hospital care when they need it. It is impossible to square the idea of widespread social distancing to protect the vulnerable with the return of schools, colleges and the necessary return to some sort of normal working by many workers.
One noticeable aspect of the approach of all these administrations has been their failure to protect the old, through their being dumped out of hospital into homes without testing or even after testing positive. None of them has made a genuine attempt to investigate and report the lessons of their failure. The traditional centralisation of power and secrecy in Britain has not been shattered by devolved administrations but reproduced. The Scottish and Stormont regimes show exactly the same tendencies to secrecy, centralisation and lack of accountability. They also show exactly the same instincts to authoritarian measures that substitute for an effective policy that goes beyond nationalist slogans.
Statistics are still paraded as proof of one jurisdiction being more successful than the other although this is fraught with difficulties and assumes that the statistics reflect the impact of respective Government measures: that it is the virus that is being controlled for either better or worse, rather than the virus determining mistaken responses to it, which is more obviously the case.
Lockdowns have been relaxed in each and the virus has flared up again, alongside dire warnings from Governments and their official advisors. In circumstances where many are asymptomatic the possibility of testing and tracing systems identifying the source of every or most infections and then closing them down, even if efficiently carried out, is unlikely. Not unless we face complete shutdown, which is not going to happen and which is now both too late and impossible to sustain in any case.
Comparisons drawn are always carefully chosen. Sweden was the comparator not to be followed, except that at the beginning of September the Irish State recorded 30.6 cases per 100,000 while the Swedes reported only 23.4.
On 19 September the death rate for the four parts of the UK were reported below:
It is clear that England has performed worst and Northern Ireland best. Scotland has done better than England, and my relatives confirmed reports that the SNP Government is getting credit for this.
Scottish nationalists claim that the dire performance of the Tory Government shows that Scottish independence is justified, and sometimes use comparisons to judge the Scottish performance poorly because of membership of the UK. So, for example, this blog damns membership because Scotland did not match the performance of some Scandinavian countries. Of course, its comparison at that time excluded Sweden.
So not only do the nationalists get to pick their comparators but they get to pick whether being worse means that Scotland should separate from the UK and being better (especially than the English) also means they should separate. If these statistics were the product of good Governance one must marvel at the so-far hidden wonders of the Stormont regime in Belfast that some believe works best when it doesn’t work at all, which it frequently doesn’t.
The Irish State in turn has been compared favourably to Northern Ireland, both of which recorded their first cases only two days apart. Crude mortality rates calculated by two economists, one from the North and one from the South, showed a mortality rate at that point in time of 44.5 per 100,000 in the North but only 35.8 in the South.
They recognise however that the majority of deaths, in what they call the first phase of the pandemic, was of the over-65s, 93.5% between March and June in the South and 92.8% in the North. They noted that a higher proportion of the population in the North is over 65 – 15.8% compared to 13.9% in the South. Adjusting for the age profile in each jurisdiction produces a mortality rate of 35.6 per 100,000 in the North (if it had the South’s population distribution – the rate in the South itself was 35.8), and the mortality rate in the South using the North’s population distribution would be 45 per 100,000 (the actual rate in the North was 44.5). So in fact not much different at all.
The following graphs show first, the daily new cases, and the following two graphs the cumulative total cases and death rate per million for a number of different countries.
The first graph shows that there are increased numbers of cases in a number of countries giving rise to the concern about a resurgence. The second graph however puts this into perspective, that growth in the cumulative number of cases is not at all as high as it was initially or in the first 50 to 100 days.
The third shows that the increase in the number of deaths has slowed even more than cases and the lines in the graph have flattened considerably. The point is not comparison between countries but the common pattern of reduced growth of both cases and especially deaths over the whole period of the pandemic. The first graph shows that this is the situation while cases have and may continue to increase in a range of countries.
The first of the following two graphs shows that across the world the number of new cases continues to grow but the second that the number of deaths is not following the same trajectory. A strategy that assumes the opposite will be increasingly exposed and indefensible.
Despite claims that Covid-19 and state responses to it are not political issues, it is clear that in every country this is not the case.
Dominic Cummings and his Government are determining the strategy in England; the centralising SNP is doing so in Scotland, and the dysfunctional Executive is doing it in the North of Ireland. The latest strategy out of Dublin makes explicit that the National Public Health Emergency Team has been downgraded and that decisions will be taken by politicians. The punitive fines being introduced in England are eminently political and make for potentially violent confrontation. That Keir Starmer supports them shows only that he will contribute to that coming confrontation. Maybe he will be looking for his old job back.
There is widespread deflation, if not complete surprise, that the incompetent mess that we are passing through has not led to more precipitate decline in Tory support in opinion polls. The ‘secret’ of course is the solid nationalist and reactionary support behind Brexit that clings to the Tories in order to deliver the promised new Jerusalem. The more Johnson fails to deliver the more some will cling.
Considerable responsibility for this must be laid at the door of the Labour Party whose previous leader acted as if a good Brexit was possible, but whose new one has collapsed into more or less criticising that the Tory deal has not been implemented. The idea that Brexit and its effects must be gotten out of the way, and Labour can then compete more effectively with the Tories afterwards, forgets that the effects of Brexit that have already been severe have only started.
At the moment the British press is full of articles that show that the real opposition to Boris Johnson comes not from the clever lawyer and stupid politician opposite but from those behind him.
This view that there is a good, or at least defensible Brexit, is held even by sections of the left who correctly opposed it in the referendum. Against all the evidence of its toxic character socialists are asked to unite against the specifically Tory Brexit. But far from the Tory Brexit being as far away as possible from the Brexit supported by the nationalist left’s Lexit, the Johnson version is exactly what they have demanded. There is no reason for these people to unite against a Tory Brexit with those socialists who supported Remain and there is no reason for the latter to renounce total opposition to Brexit when its every step is a disaster.
The other opposition comes from the nationalists of the SNP, which have always employed English nationalism to strengthen their own and are now successfully hiding their own failures over Covid by pointing to the worse failures down south. The difference is mainly presentational, with Sturgeon substituting seriousness for bombastic incoherence. It is noticeable that the growth in support for separation appears not to be based on any confidence that things will be so much better but that it couldn’t be worse.
Scottish nationalism appeared in a ‘Yes’ campaign to offer some positive solution to Scottish workers’ problems even if the experience of the SNP Government provided no grounds for such a view. The movement for it appeared more progressive than the objective itself, at least to those inside it. Its renewed support is based on a hope and a prayer that somehow an ‘independent’ capitalist Scotland, by virtue of this alone, will solve problems.
The North of Ireland shows the complete bankruptcy of nationalism. Just as England has an opposition that wants Government policy implemented (competently), and Scotland has a divided and discredited one, the regime in the North of Ireland can’t afford to have an opposition at all. In Ireland the governing parties may have to accept that the current opposition is not really an opposition and will have at some point to be trusted.
Governing parties and States have gotten accustomed to exercising control and issuing dire warnings tempered only by the knowledge that a new lockdown is unaffordable and unenforceable without money. Only the far-right has so far opposed the restrictions on civil liberties while pushing insane conspiracy theories and dangerous health edicts.
The justification for these restrictions reduces with every case that does not result in a death, while deaths of the vulnerable are their responsibility. A danger is that the right leverages legitimate opposition to repression of civil rights into acceptance or tolerance of other reactionary parts of its programme. Passivity and acceptance of the state’s increasingly unjustified repressive public health measures facilitates development of this possibility and does nothing to prepare workers for the disaster of a no-deal Brexit or, more likely, a Brexit sealed with a rotten deal.
The shared anti-Covid strategy of these Governments appears increasingly at odds with reality and is generating indifference and resentment. Socialists need an alternative view of the pandemic rooted in observable fact, one that avoids any support for undemocratic measures or calls for more restrictive lockdown. We also need to renew opposition to Brexit and expose its effects while seeking to draw attention to the bursting of its illusions. On their own, Covid-19 and Brexit would be a major threat, together the effect is multiplied. But opposition requires some coherent view of what is happening.
I watched the BBC Panorama programme on the NHS and the Government failure to prepare properly for the Covid-19 pandemic, despite warnings. It focused on its failure to stock and resupply adequate amounts of appropriate Personal Protection Equipment, and to spin the amount of PPE newly received by, for example, counting a pair of gloves as two items and including cleaning disposables as equipment.
The Tories cannot legitimately complain if they have made the NHS the centre of controversy because it is they who put it to the fore – ‘Protect the NHS’ is the slogan, with ‘success’ of its whole effort defined as the NHS not being overwhelmed by casualties of the virus. It is important we don’t buy into this.
We are implored to ‘Protect the NHS’ when it is the function of the NHS to be the last line of defence for us. Instead it has become the last place anyone wants to go. Having scared everyone by the lockdown, vast numbers of existing and prospective patients have either been told not to attend, had their treatment cancelled or postponed, or have been unable to get diagnoses and tests they badly need. The NHS isn’t dealing with them – it has been estimated that 18,000 extra deaths from cancer might result, currently around half of those recorded as dying from Coronavirus.
Not only has the NHS moved from defending us to us being exhorted to defend it, but the NHS is actually a threat, including to its own staff, over a hundred of whom have been estimated to have died from the virus. While appointments and operations are cancelled, and Emergency Department attendances have collapsed, we are invited to acclaim the empty Nightingdale hospitals and empty beds as a success! We are expected to recognise as successful an NHS that has become the site of infection and the one certain place to avoid unless you have absolutely no choice.
We are to applaud a service that has stopped being a National Health Service and become a National Covid Service following a transparently political agenda. As I have written before, we are invited to ‘Protect the NHS’ when truthfully what we are invited to protect is the Government that has so denuded the NHS of resources for so long, and made such a mess of the current outbreak, that it simply cannot cope with doing its day job and deal with the virus at the same time.
By making sure that the NHS is able cope we ensure that the cuts and their effects are hidden despite the crisis; but rather than seeing this as a grotesque choice we have been forced to accept we have been invited to greet it as ‘success’, as Johnson so glibly and cynically put it.
And we do this because the NHS is one indivisible saintly entity without a bureaucracy that heads it, or an amoral Government that directs it, that unproblematically reflects the innate compassion of humanity – despite the evidence that doctors, nurses and purchasing managers have all complained that this organisation is failing its own staff never mind those it is there to serve.
The NHS, created to put an end to dependence on charitable provision, has become the biggest charity case in the country. No doubt many people want to help, but the greatest help is not the individual resources many have had to fall back on but development of critical political consciousness.
We are supposed not to pay attention to the censorship of NHS staff who complain about their lack of protection but invited to applaud every week the protection these people are supposed to give us. We are simply to accept that cancer patients will not get their treatment because on balance they would then have their immune system too compromised if they became infected, which is only the proper choice if we already accept that they cannot be protected.
We are to ignore that the NHS has taken PPE from elderly care homes while moving infected patients from hospitals into them: ‘Protect the NHS’ does not apparently mean Protecting Social Care. Their clients’ deaths weren’t even counted in the headline daily total until very recently.
It becomes ‘pragmatic’ to downgrade the level of PPE required by NHS and care staff because the real scientific advice, unencumbered by Tory political pressure, would demand a level of PPE that the NHS cannot provide. So the ‘objective’ scientific advisors objectively become conspirators in covering up Tory austerity, neglect and incompetence.
This is a surreal world of spin and lies and suppression of facts, fairness and free expression that has worked because of fear and ignorance and lack of accountability, and because we really do rely on the NHS.
The Government has not been held to account by the Labour ‘opposition’, has only begun to face some media criticism recently, and has benefited from the social isolation of social distancing. This distancing includes distancing from reality, substituted by what Marxists call reification and alienation that amplifies the worst media influences and instincts to defer to authority. This authority would have us rally round flags standing either side of Government spokesmen who substitute for the primacy of the people clichéd totems of Britishness and itself. Real solidarity is replaced by calls to the police by snitches reporting neighbours who don’t get out to clap the NHS and its workers.
So, in Belfast we were told that 15,000 people would die but now only 1,500. We have appointments and procedures cancelled and postponed and over 70 Covid-19 beds created, that last week saw only around half occupied, while a further 200 plus have been set up. A hotel has been taken over but only one floor is so far used. Never mind, this may be ready for the next surge in September – October, which will perhaps translate as another Johnsonian ‘success’. Ring for a service and you can be told that resources are being devoted to the treatment of Covid-19. Appear in the City Hospital and find yourself inside a ‘clean’ area that unfortunately has just had red signing put up to indicate Covid-19 areas as the green signs disappear. In some locations work is hectic while in others activity has hardly been lower and there are only the rituals of infection control. Similar stories could be told across the NHS but it is all socially and politically invisible.
The NHS is a bureaucracy as well as a service, but it has become a saintly institution which it is blasphemous to criticise, and one that the Government has wrapped round itself to shield itself. In the Orwellian world of 2020 those who have spent ten years weakening it are holding up the banner of its defence against those whom it should serve and have suffered from the years of austerity inflicted on it. Just as NHS staff have been blamed for PPE shortages so patients are held responsible for its inadequacy.
It is therefore not ‘Our’ NHS. It doesn’t even belong to those who work in it. Working people should be asking themselves how all this is the case and what it is we really should be defending. Socialists should ask themselves just what a genuinely socialist service would look like. The NHS hasn’t been hijacked, it’s simply following orders
The British Government’s approach to the Coronavirus has been the subject of much, almost smug, criticism on this side of the Irish Sea. In the North nationalists, and not only they, have called for an all-island approach and rejection of the British strategy of ‘herd immunity’. Every British failure has been criticised and the response of the Irish Government lauded.
This was boosted enormously by the speech of acting Taoiseach Leo Varadkar, standing between the Tricolour and flag of the European Union, in bright contrast to the performance of Boris Johnson, sandwiched between two union flags. The serious and statesmanlike approach of Varadkar was taken as so much more apposite than the unpredictable and sometimes incoherent ramblings of the Tory leader. The two countries were adopting very different approaches and there was no doubt which was the better, even if Varadkar did a Churchill by saying ‘never will so many ask so much of so few’.
However, when all is said and done there is more than a little bollocks to such a view. There are certainly more similarities than differences, starting with the flag waving as the cover for a host of failures.
Ostensibly, the Irish approach is to avoid exposure of the population and to reprise the South Korean model of testing, contact tracing and then appropriate isolation. It has also taken more extreme measures to lockdown the population, for example by limiting outside exercise to within 2 kilometres of the home, and appearing to close down its economic activity even more drastically than the British.
The perception that this is a more responsible and sensible approach is one reason it has received popular support, although the same forces of compliance and deference apply in Ireland as much as in Britain. Rallying round together in face of the enemy is a natural response even if it is conflated with rallying round a political leadership that has done nothing to deserve it. And that is the most obvious similarity between the two countries.
But not only that. The NHS has been subject to at least a decade of underfunding and misleadership that has led it to be woefully unprepared for any crisis, never mind this one. The current Fine Gael administration is the most openly right-wing and pro-free market of all the parties, which caused it to be decisively rejected at the last general election, not least because even in an economic boom the Irish health services are seen as a mess.
In February it was reported that 677,344 cases were on the waiting list with over 12,000 left on trolleys in January, the second worst month on record. 2019 was the worst year ever for hospital overcrowding as 118,367 patients were left without beds during the year. This level of overcrowding showed that the Irish health system had insufficient capacity before the crisis and is utterly unprepared to deal with much greater demands now. The ‘Irish Times’ reported on the front page of its 9 April edition that ‘emergency care doctors have expressed concern that the peak of the most critically ill coronavirus patients has yet to hit hospitals as existing intensive care units approach full capacity.’
As for the expected surge, the chief executive of Nursing Home Ireland has said that ‘nursing homes are effectively dealing with the surge that the hospitals were expecting.’ This has led to ‘clusters’ of the virus appearing in 137 nursing homes and other residential facilities, up from 4 on 21 March. It is primarily the old who are dying, with the last reported median age of fatalities being 81. The Irish State is proving no more capable of protecting its older citizens than the British.
The Irish health system is so bad the NHS is held up as an examplar, mainly because of the gross inequality in Ireland arising from health insurance that gives you greater access than public patients.
While, just like Britain, the policy is to protect the service, both states are near the bottom of hospital beds and ICU beds per capita. The Government has hatched a deal to use private hospitals for public patients but this has led to protests from consultants that their private patients will not receive necessary treatment.
In both jurisdictions the Government has promised levels of testing that they have completely failed to deliver, which is possibly even more egregious in the case of Ireland given its so-called strategy. Johnson and his Government have gone from promising 250,000 tests a day, to promises of 100,000 by the end of the month (made at the start of it), while on 8 April Public Health England was reporting a testing capacity of 14,000.
In Ireland the Minister of Health promised 15,000 tests per day on March 19, while two weeks later the total was 1,500. Almost a week after that, Dr Jack Lambert from the Mater Hospital in Dublin was asking ‘how can you talk about flattening the curve where you’re testing such small numbers of people and people are queuing up to get testing?’
In nursing homes some tests have taken 10 days or more for results to come through. There are also reports of delays in tracing people having contact with those testing positive, making a total nonsense of the supposed strategy. Never mind, the Irish Minister of Health has promised action by the end of the month as well.
Shortages of Personal Protection Equipment exist in Ireland just as they exist in Britain, exposing health and care workers to the virus and onward transmission to the patients, clients and residents they care for. Again, the chief executive of Nursing Home Ireland has said that nursing homes are suffering severe shortages, with just 51 receiving enough, and then only for three days normal usage, while 63 others are still waiting for a delivery. Promises made by the Minister of Health to the sector have not been delivered. Not that hospitals have all they need, St Vincent’s in Dublin has warned that it is facing ‘considerable difficulty’ in sourcing masks, and that the ‘ongoing availability of masks cannot be guaranteed’.
In Britain there are numerous reports of threats to NHS staff who go to the media to explain the consequences of Government failure. Weekly clapping on behalf of NHS workers is evidence of widespread support for the service, but the silencing of NHS workers demonstrates that the NHS is not ‘our’ NHS; it is owned, run and controlled by the same state that has so abysmally failed to protect its own workers. Were the NHS really an example of socialism we would not have its workers afraid to speak out – they would own, run, and control it and be able to speak openly.
In their place we have daily press conferences, where questions routinely don’t get answered, including by the experts, while data is misleading – the figures of those infected are next to worthless and the total number dying isn’t even accurate. But at least in Britain they have daily press conferences where questions are asked, and there is a pretence at answering; the Irish Government has distinguished itself by its even greater secrecy, opposition to accountability or examination of its policies. Instead, as everywhere else, moral commands induce moral outrage as a substitute for critical engagement.
Even that voice of the restrained and sober middle class, ‘The Irish Times’, has editorialised on the difficulty of obtaining information, e.g. on waiting times for test samples, on the backlog of tests, the state’s stock of protective equipment, the real-time state of ICUs, and how the virus is interacting with other conditions. It has noted the ‘discomfort with scrutiny’ and Ministers’ requests that questions be sent in advance.
This follows the Executive’s attempt to shut down debate in the Dail, which was rejected. This, from a Government without a mandate, that has shut down large parts of the economy sending unemployment rocketing; instituted strict limits on free movement, and introduced draconian measures that give the Garda the power to arrest you for refusing to obey instructions or to give your name and address.
We are informed that the decisive intervention that ensured the Garda got such powers was the Garda itself, through the Commissioner Drew Harris, ex of the Royal Ulster Constabulary and Police Service of Northern Ireland, recalling for me that the date of birth question was always the one that refusal to answer might lead you to being lifted by the RUC.
We can see that the Irish State has done nothing to warrant either the praise or trust it has received. Yet it cannot hide forever from the inadequacies of the health system for which it is responsible. It will also not be able to make good its promise that the cost of shutting down the economy and temporarily supporting incomes will not lead to austerity further down the line. This is simply a lie.
At the same time as coronavirus has consumed attention, the politicians and media have been obsessing over the formation of a new Government, with the prospect of a coalition between the two reactionary civil war parties, ruled out so categorically, now looking more likely. The complaint of both is that no other Party wants to join them, such is the distrust. Except for Sinn Fein, which says a lot about all three.
However, rather than the problem being lack of a Government, the problem is lack of an opposition. The trade union movement is disarmed because of state subsidies for those affected by unemployment although this is unsustainable and will not be sustained. The left is in thrall to massive state intervention, which it talks and acts as if is some sort of socialism, when it is not. The authoritarian measures are opposed but not vehemently because these have not yet become unpopular. Not for the first time the potential to present an alternative is lost, because no alternative is presented.


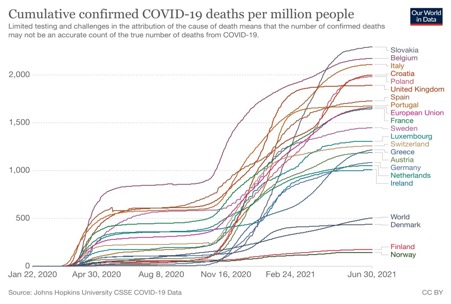


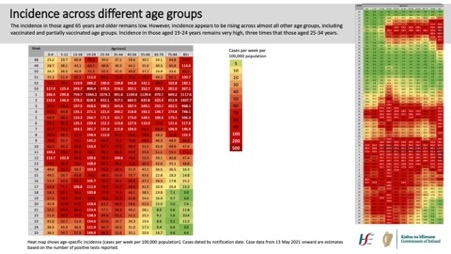
 Following ‘the science’ and its scientists that we looked at in the two previous posts does not look well in hindsight, as a short review of the course of the pandemic in the Irish State demonstrates. In the early days these were forecasting 20,000 deaths, six times the current figure which is just over 3,300, and an even greater over-estimate than the influential Imperial College paper that forecast a possible 500,000 deaths in the UK.
Following ‘the science’ and its scientists that we looked at in the two previous posts does not look well in hindsight, as a short review of the course of the pandemic in the Irish State demonstrates. In the early days these were forecasting 20,000 deaths, six times the current figure which is just over 3,300, and an even greater over-estimate than the influential Imperial College paper that forecast a possible 500,000 deaths in the UK.
 The policy of lockdowns has been approved by many on the left, with the additional argument that they have not been strict enough. Some appear to believe that pandemic induced crises necessarily open up opportunities for revolutionary crises. These are considered opportunities to mobilise the working class to resist attacks on its social position and turn it towards socialism. Crises then become both the necessary and sufficient condition for political revolution. What these sufficient and necessary conditions might actually be is not considered. That question has been answered and is no longer a question.
The policy of lockdowns has been approved by many on the left, with the additional argument that they have not been strict enough. Some appear to believe that pandemic induced crises necessarily open up opportunities for revolutionary crises. These are considered opportunities to mobilise the working class to resist attacks on its social position and turn it towards socialism. Crises then become both the necessary and sufficient condition for political revolution. What these sufficient and necessary conditions might actually be is not considered. That question has been answered and is no longer a question. The Northern Ireland Health minister was interviewed on the BBC
The Northern Ireland Health minister was interviewed on the BBC  The advice from the health experts of the National Public Health Emergency Team (NPHET) was that it was necessary to move from level 2/3 to level 5 because this was the “only opportunity” to get Covid-19 “back under control”. But when this was rejected by the government and Leo Varadkar went on TV to cut the Chief Medical Officer (CMO) off at the knees, he damned not only the CMO and his advice but also the strategy of his Government.
The advice from the health experts of the National Public Health Emergency Team (NPHET) was that it was necessary to move from level 2/3 to level 5 because this was the “only opportunity” to get Covid-19 “back under control”. But when this was rejected by the government and Leo Varadkar went on TV to cut the Chief Medical Officer (CMO) off at the knees, he damned not only the CMO and his advice but also the strategy of his Government. Just over a month ago my wife and I visited my daughter, her boyfriend, and my sister in Glasgow and had dinner in my sister’s house. Two weeks later this would not have been possible, I would have been breaking the Covid regulations; in fact, my daughter and sister couldn’t have done it together even without us. They could, however, have met together in the pub, which of course doesn’t make much sense, as this
Just over a month ago my wife and I visited my daughter, her boyfriend, and my sister in Glasgow and had dinner in my sister’s house. Two weeks later this would not have been possible, I would have been breaking the Covid regulations; in fact, my daughter and sister couldn’t have done it together even without us. They could, however, have met together in the pub, which of course doesn’t make much sense, as this 
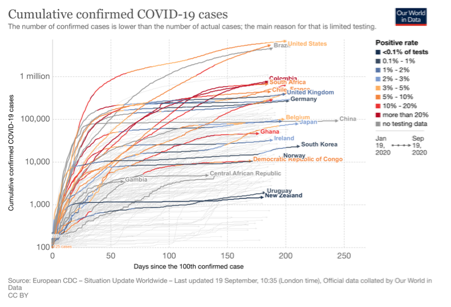
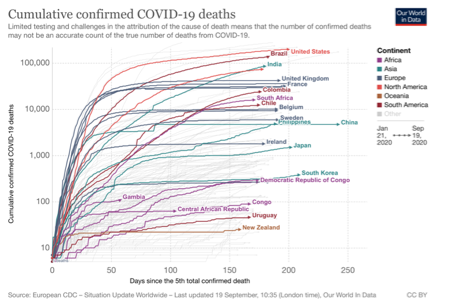 The first graph shows that there are increased numbers of cases in a number of countries giving rise to the concern about a resurgence. The second graph however puts this into perspective, that growth in the cumulative number of cases is not at all as high as it was initially or in the first 50 to 100 days.
The first graph shows that there are increased numbers of cases in a number of countries giving rise to the concern about a resurgence. The second graph however puts this into perspective, that growth in the cumulative number of cases is not at all as high as it was initially or in the first 50 to 100 days.

 I watched the BBC Panorama programme on the NHS and the Government failure to prepare properly for the Covid-19 pandemic, despite warnings. It focused on its failure to stock and resupply adequate amounts of appropriate Personal Protection Equipment, and to spin the amount of PPE newly received by, for example, counting a pair of gloves as two items and including cleaning disposables as equipment.
I watched the BBC Panorama programme on the NHS and the Government failure to prepare properly for the Covid-19 pandemic, despite warnings. It focused on its failure to stock and resupply adequate amounts of appropriate Personal Protection Equipment, and to spin the amount of PPE newly received by, for example, counting a pair of gloves as two items and including cleaning disposables as equipment. The British Government’s approach to the Coronavirus has been the subject of much, almost smug, criticism on this side of the Irish Sea. In the North nationalists, and not only they, have called for an all-island approach and rejection of the British strategy of ‘herd immunity’. Every British failure has been criticised and the response of the Irish Government lauded.
The British Government’s approach to the Coronavirus has been the subject of much, almost smug, criticism on this side of the Irish Sea. In the North nationalists, and not only they, have called for an all-island approach and rejection of the British strategy of ‘herd immunity’. Every British failure has been criticised and the response of the Irish Government lauded.