 In a recent opinion column in ‘The Irish Times’ the writer asserted that the virus ‘has always killed randomly’, proving the old adage that opinions are like arseholes – everyone’s got one. In fact, of course, Covid-19 doesn’t kill randomly and the fact that it doesn’t should be the starting point for understanding not only its effects but also how it should be dealt with. And so, in many cases, it has.
In a recent opinion column in ‘The Irish Times’ the writer asserted that the virus ‘has always killed randomly’, proving the old adage that opinions are like arseholes – everyone’s got one. In fact, of course, Covid-19 doesn’t kill randomly and the fact that it doesn’t should be the starting point for understanding not only its effects but also how it should be dealt with. And so, in many cases, it has.
For example, in this article in Nature Medicine the writers state in relation to the first wave that ‘in absolute terms, the total mortality toll of the pandemic was overwhelmingly in those aged 65 years and older, who experienced 94% of all excess deaths. In relative terms, older people were also affected more, with mortality in these ages being ~40% higher than it would have been in the absence of the pandemic in Spain and England and Wales and ~30% higher in Belgium, Scotland and Italy. The largest effect on those younger than 65 years was in England and Wales—26% (20–32%) for males and 22% (17–28%) for females—followed by Scotland, Spain, Sweden and Italy.’
It goes on to state that ‘the fourth group of countries, which experienced the highest mortality toll, consists of Belgium, Italy, Scotland, Spain and England and Wales’, which confounds the political spin that the Scottish Government did a good job.
‘The spread of infection within and between hospitals and care homes, and between them and the community, is itself an important determinant of infections and deaths in both the vulnerable groups and the general population. Where infection rates were high and care homes were not appropriately safeguarded—namely in Spain, the United Kingdom, Belgium, Italy, France and Sweden—a large number of care home residents died from confirmed or probable COVID-19. The initial seeding through discharge of infected patients to care homes was compounded by lack of testing and protective equipment for staff and residents and, especially in privately run care homes, regular movement of (temporary) staff across facilities.’
In the Irish state 93 per cent of fatalities have had an underlying condition according to the Central Statistics Office, with a median age of 83. The most common underlying condition of those who died was chronic heart disease but the relevant conditions also included kidney, liver and neurological disease as well as cancer and diabetes. In the North people aged 75 and over accounted for 78 per cent of Covid-19 related deaths in the year up to the end of October.
Health experts in Ireland, both North and South, and defenders of the lockdown approach more generally, have claimed that the only way to prevent death in these groups is a blanket lockdown that restricts everyone and justified their recent and current restrictions on this basis. But it hasn’t worked.
In yesterday’s Belfast paper, the ‘Irish News’, it was reported that there were outbreaks of the virus in 146 care homes; in September it was only 20. At the end of last week the newspaper reported that 44 per cent of deaths were accounted for by care home residents.
Yesterdays ‘Irish Times’ reported that a letter from the Irish State’s health regulator to the Department of Health asked why residents at some nursing homes where staff had tested positive had not themselves been tested. “Luckily, to date most centres are reporting that these residents are asymptomatic. However, we cannot rely on the situation continuing.” In the month of October, 39 of the 103 deaths were of residents of nursing homes, while some of these homes have made persistent complaints of inadequate support from the health service.
Defenders of universal lockdown argue that you can’t protect the vulnerable without generalised measures, but these measures mean that not only has there not been a focus on, and resources directed to, those most in need but that there can’t be.
Lockdown brings temporary reductions in cases, hospitalisation and deaths that increase when they are inevitably relaxed, which earlier in the year was modified by the warmer weather during the summer. This has led some to advocate stricter lockdowns and a ‘zero-Covid’ strategy, which sometimes doesn’t actually involve zero cases but only reduction to lower numbers so that test and trace then addresses new cases. Since the majority of cases are asymptomatic it is never explained how these could be identified, and most of them wouldn’t; which also explains why the common metric to determine the severity of restrictions – the R number – is a guess. Given the wide range of estimates of this number right from the start it should have been obvious that imprecise metrics were being employed to justify an imprecise strategy. It isn’t actually known how many people have had it or what sort of immunity has already been created.
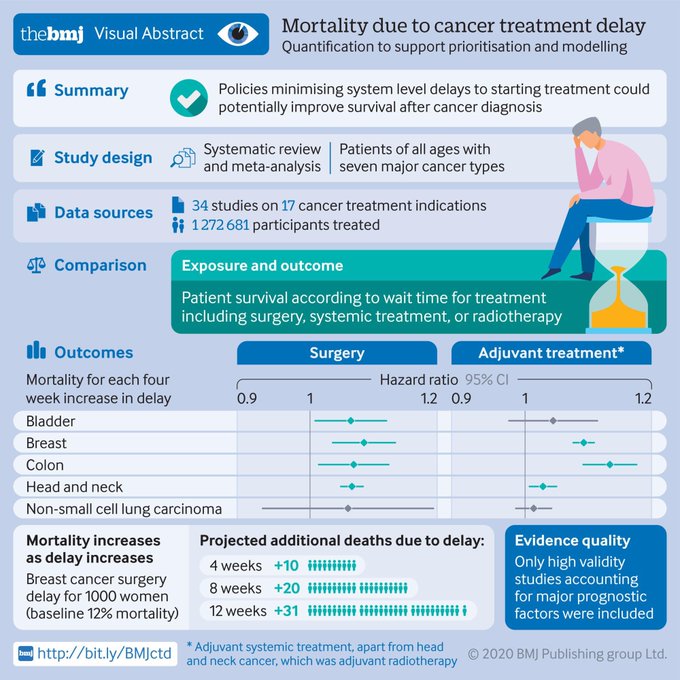
The cost of the lockdowns has been enormous and the financial cost, which will be paid by workers in the near future, has been eye-watering. The social and health cost has been less easily defined but we know it will also be huge. The Irish Hospital Consultant’s Association has estimated that almost 150,000 fewer people have had cancer screening in the first six months of this year compared to last, a drop of around 60 percent. In the North operations have been cancelled and cancer treatments delayed. The graphic at the top of this post indicates the possible fatal consequences of such delay and was tweeted by a hospital doctor in Belfast. Children’s and young people’s education has been badly damaged, domestic abuse is expected to have dramatically increased and children’s safeguarding has been endangered by the closure of schools and restricted access by healthcare professionals. Mental health is expected to have suffered, something that can only get worse over the winter.
Huge sums of money have been announced and dispersed that previously were denounced as the ravings of a lunatic Jeremy Corbyn and the left of the Labour Party. The difference however is that while the latter put forward increased spending as investment to deliver more and better jobs, the Tories have spent money to pay people to do nothing, or to pay out to their incompetent and corrupt friends through competition-free contracts.
The Left has long been aware that the best way to get people to do as they are told is to scare them, so the threat of terrorism has been used to spread fear and act as cover for attacks on democratic rights. These attacks are as nothing compared to the restrictions imposed by general lockdowns. We are invited to look down on Sweden and its policy of largely voluntary measures to restrict virus circulation and to accept that we aren’t responsible and sensible enough to do likewise – we are both too stupid and too smart. Too stupid to be trusted and too smart to try. Alternatives have come to be seen by many as the preserve of the far-right and assorted anti-science nut-jobs who sometimes deny that there is any threat at all.
The Left would normally have been expected to oppose this transparent attempt to scare the population into restrictions on their civil liberties, but instead they have joined in the moral outrage at those who aren’t doing as they are told. So young people having a rave become ‘granny killers’. They would normally have been expected to take an approach based on a materialist analysis. Instead, they have demanded that massive sectors of the economy shut up shop and their workers get paid for doing nothing, workers who are overwhelmingly young and not threatened by the virus. Pieces of paper or numbers on a computer screen are supposed to be a substitute for the production of real goods and services. Everything Marx taught about capitalism is dumped in favour of illusions in money and the state.
The alternative of an intervention through which jobs are kept, the economy can continue to function and targeted measures are taken to protect the vulnerable are labelled herd immunity as if these were some sort of swear words. The language of much of the Left has become dominated by definitions that are uttered as if they were insults. So, in Scotland, unionism and unionists are by definition reactionary. But do these words denote reaction by definition? Would the description ‘rebel’ have denoted a reactionary during the American or Spanish civil war and would socialists therefore have rejected the description ‘unionist’ or ‘loyalist’ in these struggles?
Of course, it may be said that it all depends on the context, which is precisely the point. The words herd immunity, which denote a real phenomenon, has become a term to dismiss consideration of a different way forward. Any and all speculation that acquired immunity is inadequate has been published without recognition that these objections apply equally to vaccination.
So, it has been noted that covid-specific antibodies have declined rapidly in those infected, without recognition that the immune system will have reduced these naturally because they are no longer required but will have developed the capacity to generate them again if required. The possibility of achieving some sort of herd immunity was dismissed but it has been reported in ‘The Economist’ that in Northern Italy the most badly hit places including Bergamo now enjoy some degree of immunity: ‘Serosurveys show that antibodies there are not only common, but especially so among the old and health-care workers, who need them most.’
Less reported than the possible existence of antibodies and their rapid decline has been the potential of T-cells to provide protection. This is only partly because they are harder to measure and less studied; they haven’t fitted the narrative. Except now they do.
One research project directed at health care workers in England may have found that six months after infection all the patients studied, even those who had mild symptoms, still had detectable levels of T-cells directed against the virus, even if their anti-bodies had disappeared. This, it is speculated, might be why reinfection cases seem so rare. It has been found that for some people T-cell response lasted over a decade in patients with the original SARS-COV-1 outbreak from 2002-03.
It is through seeking this type of response that the much-heralded Pfizer and BioNTech vaccine is based, and was reported in ‘The Economist’ before it became a headline in the mass media.
News of a potential vaccine doesn’t make the debate over the correct response irrelevant. There will be no mass vaccination until well into 2021, as even the Northern Ireland Health Minister has said, even if it goes through all the necessary testing and authorisation, which it hasn’t as yet. The avoidable cost of lockdown, which governments don’t seem to know how to get out of, is a big added pressure to rush vaccine approval, with all the risks this might involve.
Governments have narrowed down their options and, allied with their favoured expert advice, have given every appearance of the proverbial person who only has a hammer treating every problem as a nail. Months of potential wasteful lockdown lie ahead and the issue of targeting the vulnerable doesn’t become less important because there appears a means of protection through vaccination. Maybe then, finally, those pretending that the virus kills ‘randomly’, or that everyone has to be subject to equal treatment, will acknowledge that it doesn’t and they shouldn’t.

Great post.